

Butlletí de la societat catalana de medicina familiar i comunitària
Butlletí de la societat catalana de medicina familiar i comunitària
Butlletí de la societat catalana de medicina familiar i comunitària

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
130<br />
Revisions<br />
tenir uns criteris més restrictius, sobretot pel que fa a <strong>la</strong><br />
freqüència <strong>de</strong> presència <strong>de</strong>ls símptomes.<br />
Cap a un diagnòstic positiu<br />
Progressivament <strong>la</strong> tendència actual és <strong>la</strong> d'intentar fer<br />
un diagnòstic positiu caracteritzant <strong>la</strong> ma<strong>la</strong>ltia clínicament<br />
en una sèrie <strong>de</strong> símptomes, disminuint el nombre d'exploracions<br />
per <strong>de</strong>scartar organicitat. Això comporta addicionalment<br />
un estalvi econòmic i evita una possible iatrogènia<br />
en <strong>la</strong> pràctica d'exploracions complementaries en aquests<br />
pacients. El diagnòstic positiu té també certes limitacions<br />
que fan difícil el <strong>de</strong>senvolupament i l'ús d'aquests criteris.<br />
Per citar alguns:<br />
– Els símptomes <strong>de</strong> diferents trastorns funcionals digestius<br />
po<strong>de</strong>n superposar-se segons l'evolució clínica.<br />
– No hi ha una corre<strong>la</strong>ció fisiopatològica coneguda<br />
– El nivell sociocultural, entorn personal, <strong>familiar</strong> i <strong>la</strong>boral,<br />
pot influir a l'hora d'expressar el símptomes per<br />
part <strong>de</strong>l pacient que és amb què ens basen per c<strong>la</strong>ssificar<br />
clínicament.<br />
– No hi ha gold standard per al diagnòstic.<br />
– Degut a l'alta freqüència <strong>de</strong> trastorns funcionals<br />
digestius po<strong>de</strong>n coexistir amb altres ma<strong>la</strong>lties orgàniques<br />
digestives o no, etc.<br />
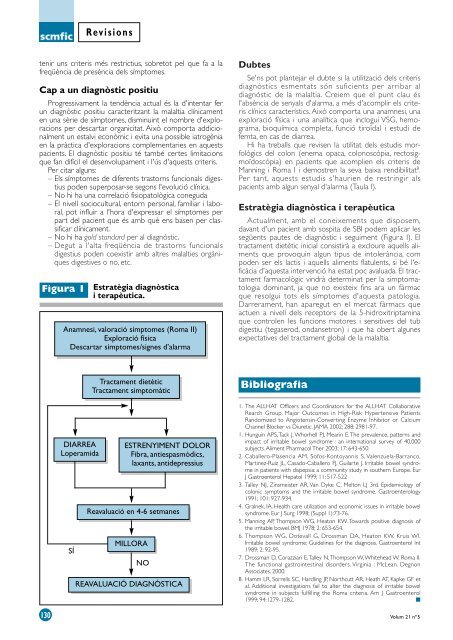
Figura 1 Estratègia diagnòstica<br />
i terapèutica.<br />
Anamnesi, valoració símptomes (Roma II)<br />
Exploració física<br />
Descartar símptomes/signes d’a<strong>la</strong>rma<br />
DIARREA<br />
Loperamida<br />
SÍ<br />
Tractament dietètic<br />
Tractament simptomàtic<br />
ESTRENYIMENT DOLOR<br />
Fibra, antiespasmòdics,<br />
<strong>la</strong>xants, anti<strong>de</strong>pressius<br />
Reavaluació en 4-6 setmanes<br />
MILLORA<br />
NO<br />
REAVALUACIÓ DIAGNÒSTICA<br />
Dubtes<br />
Se'ns pot p<strong>la</strong>ntejar el dubte si <strong>la</strong> utilització <strong>de</strong>ls criteris<br />
diagnòstics esmentats són suficients per arribar al<br />
diagnòstic <strong>de</strong> <strong>la</strong> ma<strong>la</strong>ltia. Creiem que el punt c<strong>la</strong>u és<br />
l'absència <strong>de</strong> senyals d'a<strong>la</strong>rma, a més d'acomplir els criteris<br />
clínics característics. Això comporta una anamnesi, una<br />
exploració física i una analítica que inclogui VSG, hemograma,<br />
bioquímica completa, funció tiroïdal i estudi <strong>de</strong><br />
femta, en cas <strong>de</strong> diarrea.<br />
Hi ha treballs que revisen <strong>la</strong> utilitat <strong>de</strong>ls estudis morfològics<br />
<strong>de</strong>l colon (enema opaca, colonoscòpia, rectosigmoïdoscòpia)<br />
en pacients que acomplien els criteris <strong>de</strong><br />
Manning i Roma I i <strong>de</strong>mostren <strong>la</strong> seva baixa rendibilitat 8 .<br />
Per tant, aquests estudis s'haurien <strong>de</strong> restringir als<br />
pacients amb algun senyal d'a<strong>la</strong>rma (Tau<strong>la</strong> I).<br />
Estratègia diagnòstica i terapèutica<br />
Actualment, amb el coneixements que disposem,<br />
davant d'un pacient amb sospita <strong>de</strong> SBI po<strong>de</strong>m aplicar les<br />
següents pautes <strong>de</strong> diagnòstic i seguiment (Figura I). El<br />
tractament dietètic inicial consistirà a excloure aquells aliments<br />
que provoquin algun tipus <strong>de</strong> intolerància, com<br />
po<strong>de</strong>n ser els <strong>la</strong>ctis i aquells aliments f<strong>la</strong>tulents, si bé l'eficàcia<br />
d'aquesta intervenció ha estat poc avaluada. El tractament<br />
farmacològic vindrà <strong>de</strong>terminat per <strong>la</strong> simptomatologia<br />
dominant, ja que no existeix fins ara un fàrmac<br />
que resolgui tots els símptomes d'aquesta patologia.<br />
Darrerament, han aparegut en el mercat fàrmacs que<br />
actuen a nivell <strong>de</strong>ls receptors <strong>de</strong> <strong>la</strong> 5-hidroxitriptamina<br />
que controlen les funcions motores i sensitives <strong>de</strong>l tub<br />
digestiu (tegaserod, ondansetron) i que ha obert algunes<br />
expectatives <strong>de</strong>l tractament global <strong>de</strong> <strong>la</strong> ma<strong>la</strong>ltia.<br />
Bibliografia<br />
1. The ALLHAT Officers and Coordinators for the ALLHAT Col<strong>la</strong>borative<br />
Rearch Group. Major Outcomes in High-Risk Hypertensive Patients<br />
Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium<br />
Channel Blocker vs Diuretic. JAMA 2002; 288: 2981-97.<br />
1. Hunguin APS,Tack J, Whorhell PJ, Mearin E.The prevalence, patterns and<br />
impact of irritable bowel syndrome : an international survey of 40,000<br />
subjects. Aliment Pharmacol Ther 2003; 17: 643-650.<br />
2. Caballero-P<strong>la</strong>sencia AM, Sofos-Kontoyannis S, Valenzue<strong>la</strong>-Barranco,<br />
Martinez-Ruiz JL, Casado-Caballero FJ, Gui<strong>la</strong>rte J. Irritable bowel syndrome<br />
in patients with dispepsia: a community study in southern Europe. Eur<br />
J Gastroenterol Hepatol 1999; 11: 517-522<br />
3. Talley NJ, Zinsmeister AR, Van Dyke C, Melton LJ 3rd. Epi<strong>de</strong>miology of<br />
colonic symptoms and the irritable bowel syndrome. Gastroenterology<br />
1991; 101: 927-934.<br />
4. Gralnek, IA. Health care utilization and economic issues in irritable bowel<br />
syndrome. Eur J Surg 1998; (Suppl 1):73-76.<br />
5. Manning AP, Thompson WG, Heaton KW. Towards positive diagnosis of<br />
the irritable bowel. BMJ 1978; 2: 653-654.<br />
6. Thompson WG, Dotevall G, Drossman DA, Heaton KW, Kruis WI.<br />
Irritable bowel syndrome: Gui<strong>de</strong>lines for the diagnosis. Gastroenterol Int<br />
1989; 2: 92-95.<br />
7. Drossman D, Corazziari E,Talley N,Thompson W, Whitehead W. Roma II.<br />
The functional gastrointestinal disor<strong>de</strong>rs. Virginia : McLean. Degnon<br />
Associates, 2000.<br />
8. Hamm LR, Sorrells SC, Hardling JP, Northcutt AR, Heath AT, Kapke GF et<br />
al. Additional investigations fail to alter the diagnosis of irritable bowel<br />
syndrome in subjects fulfilling the Roma criteria. Am J Gastroenterol<br />
1999; 94:1279-1282. ■<br />
Volum 21 nº5
