Beckwith-Wiedemann syndrome Hypoglossal nerve injury ... - MDC
Beckwith-Wiedemann syndrome Hypoglossal nerve injury ... - MDC
Beckwith-Wiedemann syndrome Hypoglossal nerve injury ... - MDC

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
39-year-old woman presented complaining of a 1-day history of vomiting and abdominal pain.<br />
She had had three or four episodes, with no infective prodrome. She was a physiotherapist and<br />
a competent long-distance runner; 2 days earlier she had run a 5 km race, and that morning<br />
had done her daily exercise workout. On examination there were no physical signs other than<br />
sinus tachycardia. Within 2 h, she collapsed and was moribund in acute cardiogenic shock.<br />
Chest radiography showed pulmonary congestion. Transthoracic echocardiography showed a<br />
slightly dilated, poorly functioning heart with no pericardial effusion. Cardiac catheterisation was<br />
done to exclude coronary artery disease, and an intra-aortic balloon pump was placed for<br />
circulatory support. She had no arrhythmias. Acute myocarditis was suspected and she was<br />
transferred to our cardiothoracic centre. She arrived 8 h after first presentation, was found to be<br />
in extremis, with fixed mottling of her trunk and limbs and hypotension despite epinephrine<br />
infusing at >1 µg/kg per min. She was anuric, profoundly acidaemic, and hypoxic on 100%<br />
oxygen (PaO2 6·1 kPa, pH 6·9, lactate 16 mmol/L, base excess −13). The heart was tense and<br />
dilated and a myocardial biopsy sample was taken from the left ventricle. Central veno-arterial<br />
extracorporeal membrane oxygenation (ECMO) was established; a cannula was inserted via<br />
the abdominal wall into the right atrium to drain systemic venous blood into the ECMO pump,<br />
which returned oxygenated blood via a separate cannula into the ascending aorta<br />
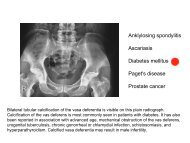
CT of the abdomen showed a large left adrenal mass (5×6 cm).<br />
Left adrenalectomy was done (day 3) with concurrent ECMO<br />
support. Subsequent echocardiography showed recovering<br />
biventricular function (day 5) and ECMO was discontinued.