Full text - Journal of the Intensive Care Society
Full text - Journal of the Intensive Care Society
Full text - Journal of the Intensive Care Society

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
© The <strong>Intensive</strong> <strong>Care</strong> <strong>Society</strong> 2012<br />
Airway injury and haemorrhage<br />
associated with <strong>the</strong> Frova intubating<br />
introducer<br />
JA Simpson, M Duffy<br />
Introduction<br />
Although <strong>the</strong> Eschmann tracheal tube Introducer (Smiths<br />
Medical, Ashford, UK) was once considered <strong>the</strong> gold standard<br />
for assisting intubation, concerns about cross-infection with<br />
multiple-use devices 1,2 have led to an increasing reliance upon<br />
single-use alternatives. 3 The Frova intubating introducer<br />
(bougie) (Cook ® Medical, Bloomington, USA) is a commonly<br />
used example and has a high success rate for tracheal<br />
intubation in manikins. 4-6 There may be however increased<br />
potential for tissue trauma, suggested by both manikin<br />
studies 4,5 and case reports in <strong>the</strong> literature. 7-12 In common with<br />
airway exchange ca<strong>the</strong>ters, 13,14 high-pressure source ventilation<br />
via <strong>the</strong> hollow lumen <strong>of</strong> <strong>the</strong> Frova intubating introducer may<br />
also lead to barotrauma. 15<br />
Case report<br />
A 49-year-old man with pancreatitis secondary to alcohol was<br />
admitted to <strong>the</strong> intensive care unit (ICU) with multiple organ<br />
failure. Although baseline tests <strong>of</strong> coagulation (prothrombin<br />
and activated partial thromboplastin times) were within normal<br />
ranges, he had thrombocytopenia. Following a platelet<br />
transfusion, which increased <strong>the</strong> platelet count from 18 to<br />
26 × 109 /L, a wide-bore double-lumen haem<strong>of</strong>iltration ca<strong>the</strong>ter<br />
was inserted into <strong>the</strong> right internal jugular vein. Continuous<br />
veno-veno haem<strong>of</strong>iltration was <strong>the</strong>n commenced without<br />
anticoagulation. Attempts to control <strong>the</strong> patient’s confusion<br />
and agitation with light sedation led to hypoxia despite airway<br />
manoeuvres to alleviate upper airway obstruction. Peripheral<br />
oxygen saturations fell to 76% with a PaO2 measured at<br />
6.3 kPa on 15 L/min oxygen via an oxygen mask with a<br />
reservoir bag. The decision was taken to perform a rapid<br />
sequence intubation and to initiate mechanical ventilation.<br />
Body mass index was 28 kg/m2 and, following airway<br />
assessment, difficult intubation was not anticipated.<br />
Case reports<br />
Airway trauma is a recognised complication <strong>of</strong> tracheal intubation when using an intubating introducer. We report such a<br />
case in which a Frova TM intubating introducer (bougie) traumatised <strong>the</strong> intermediate bronchus, at <strong>the</strong> junction <strong>of</strong> <strong>the</strong> right<br />
middle and inferior lobar bronchi. This caused major tracheobronchial haemorrhage and hypoxia. The injury resulted in<br />
formation <strong>of</strong> a flap <strong>of</strong> tissue, which <strong>the</strong>n obstructed <strong>the</strong> right middle and inferior bronchi with a ball-valve effect. We<br />
discuss <strong>the</strong> relevant literature and explore o<strong>the</strong>r contributory factors to this life-threatening complication.<br />
Keywords: intubation; airway management; trauma; disposable equipment; haemorrhage<br />
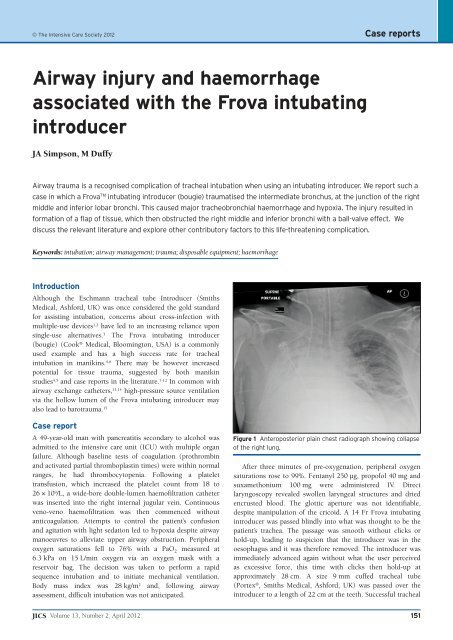
Figure 1 Anteroposterior plain chest radiograph showing collapse<br />
<strong>of</strong> <strong>the</strong> right lung.<br />
After three minutes <strong>of</strong> pre-oxygenation, peripheral oxygen<br />
saturations rose to 99%. Fentanyl 250 µg, prop<strong>of</strong>ol 40 mg and<br />
suxamethonium 100 mg were administered IV. Direct<br />
laryngoscopy revealed swollen laryngeal structures and dried<br />
encrusted blood. The glottic aperture was not identifiable,<br />
despite manipulation <strong>of</strong> <strong>the</strong> cricoid. A 14 Fr Frova intubating<br />
introducer was passed blindly into what was thought to be <strong>the</strong><br />
patient’s trachea. The passage was smooth without clicks or<br />
hold-up, leading to suspicion that <strong>the</strong> introducer was in <strong>the</strong><br />
oesophagus and it was <strong>the</strong>refore removed. The introducer was<br />
immediately advanced again without what <strong>the</strong> user perceived<br />
as excessive force, this time with clicks <strong>the</strong>n hold-up at<br />
approximately 28 cm. A size 9 mm cuffed tracheal tube<br />
(Portex ® , Smiths Medical, Ashford, UK) was passed over <strong>the</strong><br />
introducer to a length <strong>of</strong> 22 cm at <strong>the</strong> teeth. Successful tracheal<br />
JICS Volume 13, Number 2, April 2012 151
Case reports<br />
placement was confirmed by capnography, bilateral chest wall<br />
movement and ausculation <strong>of</strong> both lung fields. The patient’s<br />
lungs were ventilated with 100% oxygen and oxygen<br />
saturations rose from 88% to 99%.<br />
After a fur<strong>the</strong>r 10 minutes, oxygen saturations fell again,<br />
from 99% to 84%. Auscultation <strong>of</strong> <strong>the</strong> chest revealed reduced<br />
breath sounds on <strong>the</strong> right. An anteroposterior plain chest<br />
radiograph was performed (Figure 1) which demonstrated<br />
collapse <strong>of</strong> <strong>the</strong> right lung and an adequately positioned tracheal<br />
tube. Immediate flexible fibreoptic bronchoscopy revealed<br />
blood throughout <strong>the</strong> right bronchial tree with active<br />
haemorrhage. Suction improved ventilation to <strong>the</strong> right upper<br />
lobe. An intraluminal flap <strong>of</strong> tissue, lacerated from <strong>the</strong> wall <strong>of</strong><br />
<strong>the</strong> intermediate bronchus, was noted to be causing ongoing<br />
obstruction to <strong>the</strong> right middle and inferior bronchi with a<br />
ball-valve effect (Figures 2a and 2b). Fur<strong>the</strong>r extensive<br />
suctioning <strong>of</strong> <strong>the</strong> right bronchial tree was performed. After<br />
transfusion <strong>of</strong> two fur<strong>the</strong>r pools, <strong>the</strong> platelet count increased to<br />
63 × 10 9 /L and <strong>the</strong> bleeding stopped.<br />
152<br />
2a<br />
2b<br />
Figures 2a and b Intra-luminal flap <strong>of</strong> tissue obstructing <strong>the</strong><br />
right middle and inferior bronchi with a ball-valve effect.<br />
Figure 3 Anteroposterior plain chest radiograph showing partial<br />
improvement, one hour after flexible bronchoscopy.<br />
Figure 4 Anteroposterior plain chest radiograph showing linear<br />
atelectasis at <strong>the</strong> right base, two months after discharge from<br />
hospital.<br />
The patient was paralysed and ventilated with a lung<br />
protective strategy. Oxygenation and radiographic appearances<br />
(Figure 3) improved significantly over <strong>the</strong> subsequent hours.<br />
In view <strong>of</strong> this, he was managed conservatively following<br />
advice from a thoracic surgeon at 12 hours. His trachea was<br />
extubated three days later. He was discharged from ICU after a<br />
fur<strong>the</strong>r three days and from hospital after two weeks. The plain<br />
chest radiograph continued to improve (Figure 4) and he made<br />
a full recovery.<br />
Discussion<br />
Airway complications confer high mortality and morbidity in<br />
critically ill patients. 13 These patients are at particular risk <strong>of</strong><br />
iatrogenic injury16 and complications such as oesophageal<br />
intubation and failed rescue techniques are more common. 13<br />
This case demonstrates several issues related to <strong>the</strong>ir<br />
management.<br />
Volume 13, Number 2, April 2012 JICS
Significant airway trauma can result from <strong>the</strong> use <strong>of</strong> airway<br />
adjuncts such as <strong>the</strong> Frova intubating introducer, 7-13 even when<br />
used with what <strong>the</strong> user perceives to be minimal force.<br />
Although it has a high success rate for tracheal intubation, 7<br />
manikin studies have shown it to exert a greater force at its tip<br />
compared to <strong>the</strong> Eschmann tracheal tube introducer, 4,5 which<br />
may result in increased potential for tissue damage. 9,10 This is<br />
especially relevant when hold-up is used to detect tracheal<br />
placement, 7 which has led to <strong>the</strong> suggestion that it should only<br />
be sought in <strong>the</strong> absence <strong>of</strong> clicks. 7,10 Iatrogenic airway trauma<br />
associated with bougies (type not clarified) and airway<br />
exchange ca<strong>the</strong>ters was recognised as a cause <strong>of</strong> morbidity in<br />
<strong>the</strong> 4th National Audit Project (NAP4) <strong>of</strong> <strong>the</strong> Royal College <strong>of</strong><br />
Anaes<strong>the</strong>tists and Difficult Airway <strong>Society</strong> (DAS). 13 The NAP4<br />
authors recommended that when using airway exchange<br />
ca<strong>the</strong>ters, <strong>the</strong> tip should not reach <strong>the</strong> carina (ie it should be<br />
inserted to a maximum distance <strong>of</strong> 26 cm at <strong>the</strong> lips) and when<br />
using bougies ‘great care should be taken to avoid using<br />
excessive force.’ 13<br />
Concerns about cross-infection with multiple-use devices<br />
have led to an increasing use <strong>of</strong> single-use alternatives. 3<br />
However, if <strong>the</strong> performance <strong>of</strong> single-use alternatives is<br />
inferior, <strong>the</strong>re is clearly a balance to be struck between <strong>the</strong> risk<br />
to patients from cross-infection and <strong>the</strong> risk to patients from<br />
using substandard equipment. 17 The current recommendation<br />
from <strong>the</strong> Association <strong>of</strong> Anaes<strong>the</strong>tists <strong>of</strong> Great Britain and<br />
Ireland is that single-use devices are used where appropriate,<br />
with <strong>the</strong> balance <strong>of</strong> risk requiring ‘local determination based on<br />
an assessment <strong>of</strong> patient safety, <strong>the</strong> available facilities and cost.’ 3<br />
Conclusion<br />
As <strong>the</strong> use <strong>of</strong> disposable equipment grows, it is necessary to<br />
ensure that performance and safety pr<strong>of</strong>iles are properly<br />
benchmarked against established gold standards. It is also<br />
important that devices are used in a manner that minimises <strong>the</strong><br />
risk <strong>of</strong> patient harm. The Frova intubating introducer is an<br />
effective device4-7 and has obvious advantages in terms <strong>of</strong><br />
infection control. However its potential to cause tissue<br />
damage, 8-12 particularly in association with hold-up, 7 is <strong>of</strong><br />
concern. There must always be a willingness to adapt practice<br />
as traditional techniques may not translate to single-use<br />
equipment. However, as <strong>the</strong> Frova intubating introducer<br />
instructions for use state, it ‘should not be advanced past <strong>the</strong><br />
carina,’ 18 it cannot be used when following <strong>the</strong> current DAS<br />
guidelines19 for difficult tracheal intubation, in which using<br />
hold-up is a recommended technique.<br />
Acknowledgement<br />
Published with <strong>the</strong> written consent <strong>of</strong> <strong>the</strong> patient.<br />
Competing interest<br />
No external funding and no competing interests declared.<br />
Commentary:<br />
Drs Simpson and Duffy’s case report illustrates several<br />
points. Firstly, <strong>the</strong> case illustrates how critically ill patients<br />
References<br />
Case reports<br />
1. Le<strong>the</strong>ren M. Sterilisation <strong>of</strong> gum elastic bougies. Anaes<strong>the</strong>sia 1994;49:921.<br />
2. Jerwood DC, Mortili D. Disinfection <strong>of</strong> gum elastic bougies. Anaes<strong>the</strong>sia<br />
1995;50:376.<br />
3. Association <strong>of</strong> Anaes<strong>the</strong>tists <strong>of</strong> Great Britain and Ireland (AAGBI).<br />
AAGBI Safety Guideline: Infection control in Anaes<strong>the</strong>sia. Anaes<strong>the</strong>sia<br />
2008;63:1027-36.<br />
4. Hodzovic I, Latto IP, Wilkes AR et al. Evaluation <strong>of</strong> Frova, single-use<br />
intubation introducer, in a manikin. Comparison with Eschmann<br />
multiple-use introducer and Portex single-use introducer. Anaes<strong>the</strong>sia<br />
2004;59:811-16.<br />
5. Janakiraman C, Hodzovic I, Reddy S et al. Evaluation <strong>of</strong> tracheal tube<br />
introducers in simulated difficult intubation. Anaes<strong>the</strong>sia 2009;64:309-14.<br />
6. Whitcombe A, Strang T. A comparison <strong>of</strong> multiple-use and single-use<br />
bougies. Anaes<strong>the</strong>sia 2005;60:416-17.<br />
7. Hodzovic I, Wilkes AR, Stacey M et al. Evaluation <strong>of</strong> clinical<br />
effectiveness <strong>of</strong> <strong>the</strong> Frova single-use tracheal tube introducer. Anaes<strong>the</strong>sia<br />
2008;63:189-94.<br />
8. Vila Caral P, Castillo Omedas R, Llubiá Maristany C. Laceración<br />
traqueal durante la intubación traqueal con guía de intubación Frova.<br />
Revista Espanola de Anestesiologia y Reanimacion 2010;57:599-602.<br />
9. Umesh G, Jasvinder K. Frova introducer for tracheal intubation – our<br />
comments and experience. Anaes<strong>the</strong>sia 2008;63:1260-61.<br />
10.Hodzovic I, Wilkes AR, Stacey M et al. Frova introducer for tracheal<br />
intubation – our comments and experience [a reply]. Anaes<strong>the</strong>sia<br />
2008;63:1261-62.<br />
11.Hodzovic I, Latto IP. Singe-use introducers may not be fit for purpose.<br />
Anaes<strong>the</strong>sia 2007;62:1189-90.<br />
12.Evans H, Hodzovic I, Latto IP. Tracheal tube introducers: choose and use<br />
with care. Anaes<strong>the</strong>sia 2010;65:859.<br />
13.Cook TM, Woodall N, Frerk C. Fourth National Audit Project <strong>of</strong> <strong>the</strong><br />
Royal College <strong>of</strong> Anaes<strong>the</strong>tists and <strong>the</strong> Difficult Airway <strong>Society</strong>: Major<br />
Complications <strong>of</strong> Airway Management in <strong>the</strong> United Kingdom. BJA<br />
2011;106:632-42.<br />
14.Scottish Courts Fatal Accident Enquiry into <strong>the</strong> death <strong>of</strong> Gordon Ewing.<br />
Glasgow, April 2010; www.scotcourts.gov.uk/opinions/2010FAI15.html<br />
(accessed 27th Jan 2012).<br />
15.Rao A, Webster L, Turner M. Bougie induced airway trauma. Presented at<br />
<strong>the</strong> Difficult Airway <strong>Society</strong> Annual Congress, Cheltenham 2010;Poster<br />
83C<br />
16.Rothschild JM, Landrigan CP, Cronin JW et al. The Critical <strong>Care</strong> Safety<br />
Study: The incidence and nature <strong>of</strong> adverse events and serious medical<br />
errors in intensive care. Crit <strong>Care</strong> Med 2005;33:1694-700.<br />
17.Rowley E, Dingwall R. The use <strong>of</strong> single-use devices in anaes<strong>the</strong>sia:<br />
balancing <strong>the</strong> risks to patient safety. Anaes<strong>the</strong>sia 2007;62:569-74.<br />
18.Frova Intubating Introducer Data Sheet. Cook ® Medical, Bloomington,<br />
USA.<br />
19.Henderson JJ, Popat MT, Latto IP. Difficult Airway <strong>Society</strong> guidelines for<br />
management <strong>of</strong> <strong>the</strong> unanticipated difficult intubation. Anaes<strong>the</strong>sia<br />
2004;59:675-94.<br />
James A Simpson Registrar in Anaes<strong>the</strong>sia<br />
james.simpson2@nhs.net<br />
Mike R Duffy Consultant in Anaes<strong>the</strong>sia and <strong>Intensive</strong> <strong>Care</strong><br />
Derriford Hospital, Plymouth<br />
are at increased risk <strong>of</strong> major sequelae when complications <strong>of</strong><br />
airway management occur. The 4th National audit project <strong>of</strong><br />
JICS Volume 13, Number 2, April 2012 153
Case reports<br />
<strong>the</strong> Royal College <strong>of</strong> Anaes<strong>the</strong>tists and Difficult Airway <strong>Society</strong><br />
has hopefully made it clear that airway management in <strong>the</strong> ICU<br />
must be treated with great respect.<br />
Secondly we must choose and use airway equipment<br />
carefully. There is a wide array <strong>of</strong> bougies, introducers and<br />
airway exchange ca<strong>the</strong>ters (AECs) available and most ICUs<br />
will possess several. They vary in length, stiffness, shape and<br />
rigidity <strong>of</strong> <strong>the</strong> tip and also in intended purpose. All users<br />
should familiarise <strong>the</strong>mselves before using <strong>the</strong>m, including<br />
reading <strong>the</strong> instructions for use.<br />
Finally, <strong>the</strong>re is a more specific lesson to learn.<br />
Tracheobronchial trauma during intubation is a serious<br />
complication. Subsequent positive pressure may compound <strong>the</strong><br />
injury. If a bougie or AEC is advanced beyond <strong>the</strong> carina, <strong>the</strong><br />
risk <strong>of</strong> bronchial damage and <strong>of</strong> <strong>the</strong> device wedging in <strong>the</strong><br />
airway increases. If pressure is applied through <strong>the</strong> lumen <strong>of</strong> a<br />
wedged device, especially if a high-pressure source is used,<br />
<strong>the</strong>re will be no route <strong>of</strong> egress for <strong>the</strong> gas and barotrauma is<br />
almost inevitable. The case <strong>of</strong> Gordon Ewing is a potent<br />
example <strong>of</strong> this (see Sherriff Ruxton’s report into his death<br />
154<br />
http://www.scotcourts.gov.uk/opinions/2010FAI15.html )<br />
Such injuries can be vastly reduced by three simple actions:<br />
A bougie or AEC should never be inserted beyond 26 cm<br />
from <strong>the</strong> lips (mid-trachea). Attaching tape as a marker at<br />
26 cm is useful, but manufacturers could act on this too by<br />
marking devices with <strong>the</strong> maximum insertion depth.<br />
It is rarely, if ever, necessary to deliver oxygen through a<br />
bougie/AEC. The devices can be used only for passage <strong>of</strong> a<br />
tracheal tube, it takes but a few seconds. Their use as<br />
oxygenating devices should be reserved for life-threatening<br />
situations.<br />
No force should ever be applied to <strong>the</strong> bougie when it holds<br />
up (at whatever level), and <strong>the</strong>re is an argument that holdup<br />
should not be used as a sign <strong>of</strong> tracheal insertion at all.<br />
Tim Cook Consultant in Anaes<strong>the</strong>sia and <strong>Intensive</strong> <strong>Care</strong><br />
Medicine, Bath<br />
timcook007@googlemail.com<br />
Volume 13, Number 2, April 2012 JICS