Lacrimal Canaliculitis, A Case Report - KSOS
Lacrimal Canaliculitis, A Case Report - KSOS
Lacrimal Canaliculitis, A Case Report - KSOS

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
December 2008 M. Chakrabarti et al. - Ocular Contusion Injury 421<br />
<strong>Lacrimal</strong> <strong>Canaliculitis</strong>, A <strong>Case</strong> <strong>Report</strong><br />
Dr. Bindu N. Das MS, Dr. Sisira MS<br />
Introduction<br />
<strong>Canaliculitis</strong> is a chronic unilateral infection of the<br />
lacrimal canaliculus which is often overlooked and<br />
treated unsatisfactorily. Bacteria, fungi and viruses may<br />
all produce such infection , the most common agents<br />
reported being actinomyces. Here we report a case of<br />
culture positive bilateral actinomyces canaliculitis<br />
involving both upper and lower puncti.<br />
<strong>Case</strong> <strong>Report</strong><br />
A 40 year old male patient presented to us with<br />
complaints of watering and purulent discharge from<br />
left eye of 1 year duration, pain and swelling of the left<br />
eyelids for 2 months. On examination his vision was<br />
6/6 in right eye and 6/12 in left eye. Examination of<br />
left eye showed a tender fusiform swelling in the medial<br />
one third of left upper and lower eyelids. The<br />
neighbouring part of the conjunctiva was inflammed.<br />
(Fig.1) There was no tenderness and swelling in the<br />
lacrimal sac area. The upper and lower puncti were<br />
found to be pouting with expression of tenacious pus<br />
on pressure over the swelling. The right eye also showed<br />
pouting of lower puncta though it did not show<br />
swelling. Patient was asymptomatic in the right eye.<br />
Rest of the anterior and posterior segment was normal.<br />
He was a known diabetic on irregular treatment.<br />
The punctum was split under topical anaesthesia using<br />
a fine scissors taking aseptic precautions and a thick,<br />
tenacious purulent material was expressed from the<br />
canaliculus. (Fig.2) The casts were removed by<br />
performing a 3- snip procedure (Fig.3) followed by<br />
irrigation with penicillin solution (100, 000 units). The<br />
patient was also treated with fortified penicillin eye<br />
drops and a course of oral penicillin. The casts collected<br />
were sent for microbiological investigations. Repeated<br />
irrigation with crystalline penicillin drops was done in<br />
the right eye. A portion of collected material was<br />
inoculated on blood agar and brain heart infusion broth.<br />
On Gram staining the organisms appeared as gram-<br />
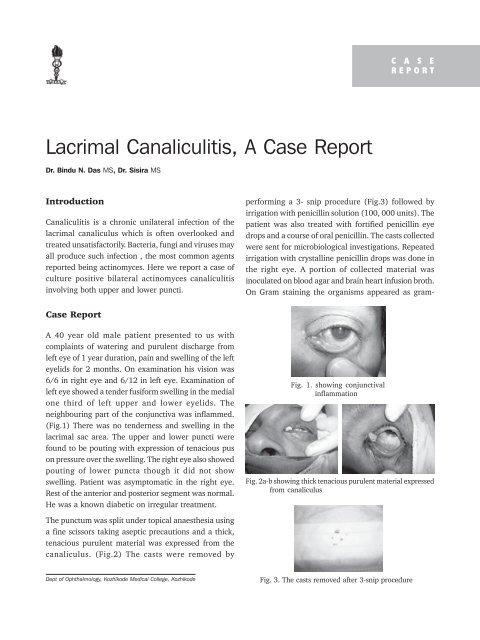
Fig. 1. showing conjunctival<br />
inflammation<br />
Fig. 2a-b showing thick tenacious purulent material expressed<br />
from canaliculus<br />
Dept of Ophthalmology, Kozhikode Medical College, Kozhikode Fig. 3. The casts removed after 3-snip procedure<br />
C A S E<br />
REPORT
422 Kerala Journal of Ophthalmology Vol. XX, No. 4<br />
Fig. 4. showing positive<br />
beaded, coccoid, thin<br />
branching filaments<br />
on gram staining<br />
positive beaded, coccoid, thin branching filaments.<br />
(Fig.4) The patient recovered rapidly and was left with<br />
a slit punctum and adjoining canaliculus. The remaining<br />
portion of the lower canaliculus was intact and was<br />
patent. Post-operatively, the swelling, conjunctivitis and<br />
discharge disappeared (Fig.5).<br />
Discussion<br />
Fig. 5. P ost-operative<br />
appearance of the eye<br />
Actinomyces israelii species is a gram-positive, castforming,<br />
non–acid-fast, non–spore-forming anaerobic<br />
bacillus. Its filamentous growth and mycelia like<br />
colonies have a striking resemblance to fungi. They are<br />
soil organisms, often found in decaying organic matter<br />
(eg, wet hay, straw). It is primarily a commensal<br />
microbe found in normal oral cavities, in tonsillar<br />
crypts, in dental plaques, and in caries teeth and enters<br />
the lacrimal system through the nasal passage or<br />
indirectly by means of saliva into the conjunctiva. The<br />
anaerobic environment also helps in the growth of the<br />
Actinomyces in the canaliculus.<br />
Other ocular manifestations include keratitis,<br />
conjunctivitis, blepharitis, dacryocystitis, postsurgical<br />
endophthalmitis, and infected porous orbital implant.<br />
Cervico-facial actinomycosis has also been reported.<br />
<strong>Canaliculitis</strong> usually presents as chronic watering,<br />
redness and discharge from eye. A pouted punctum is<br />
clinically diagnostic, although it occurs in less than<br />
50 % of all patients who are affected. Typically, the<br />
discharge is particulate and contains concretions.The<br />
plica may be swollen and congested, and canalicular<br />
swelling and overlying lid erythema are often<br />
present.The lower lid is more commonly affected, and<br />
the lacrimal sac and the duct are usually not<br />
involved.The disease is most commonly unilateral.<br />
Among the reported cases almost all were unilateral,<br />
involving the lower lid. Bilateral and upperlid<br />
involvement as in this case is a rare presentation.<br />
Concretions on the lacrimal canaliculus can also be due<br />
to Candida albicans , Aspergillus niger , Fusobacterium<br />
species, and Nocardia asteroids.<br />
Lab Studies<br />
Canalicular discharge and canaliculiths may be sent for<br />
the following studies:<br />
Gram stain/Giemsa stain<br />
Culture and sensitivity (ie, blood agar, Sabouraud,<br />
anaerobic media)<br />
Special stains (ie, calcofluor white)<br />
Treatment<br />
Actinomycetes are usually susceptible to penicillins and<br />
cephalosporins.<br />
Surgical Care<br />
Failure of resolution of canaliculitis by topical treatment<br />
necessitates surgical exploration of the canalicular<br />
system and removal of any casts. Extensive surgery is<br />
not always required. A 2-snip punctoplasty, cast<br />
removal, curettage, and probing is usually done.<br />
Subsequent lacrimal irrigation with 1 MU of penicillin<br />
in 10 mL of sterile water may be helpful.<br />
References<br />
1. Jordan DR. Dacryoadenitis, Dacryocystitis, and<br />
<strong>Canaliculitis</strong>, chapter 57. In: Cornea- Cornea and<br />
External Disease: Clinical Diagnosis and Management.<br />
Krachmer JH, Mannis MJ, Holland EJ, Eds. (St. Louis,<br />
Mosby). 1997;687-693.<br />
2. Richards WW. Actinomycotic lacrimal canaliculitis.<br />
American J Ophthalmol 1975;75:155-157.<br />
3. Pine L, Hardin H, Turner L, Roberts SS. Actinomycotic<br />
lacrimal canaliculitis - A report of two cases with a<br />
review of the characteristics which identify the causal<br />
organism. American J Ophthalmol 1960;49:1278-1298.<br />
4. Sridhar MS, Gopinathan U, Garg P, Sharma S, Rao GN.<br />
Ocular Nocardia infections with special emphasis on<br />
the cornea. Surv Ophthalmol 2001;45:361-378.<br />
5. Sharma S. Ocular Microbiology. 1st ed. (Aravind Eye<br />
Hospitals Publication, Madurai) 1988:79-84.