

ACC/AHA 2007 guideline update for the
ACC/AHA 2007 guideline update for the
ACC/AHA 2007 guideline update for the

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
e194 Circulation August 14, <strong>2007</strong><br />
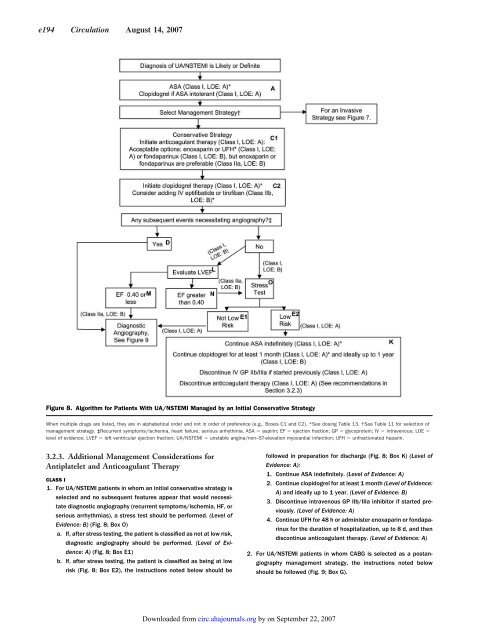
Figure 8. Algorithm <strong>for</strong> Patients With UA/NSTEMI Managed by an Initial Conservative Strategy<br />
When multiple drugs are listed, <strong>the</strong>y are in alphabetical order and not in order of preference (e.g., Boxes C1 and C2). *See dosing Table 13. †See Table 11 <strong>for</strong> selection of<br />
management strategy. ‡Recurrent symptoms/ischemia, heart failure, serious arrhythmia. ASA aspirin; EF ejection fraction; GP glycoprotein; IV intravenous; LOE <br />
level of evidence; LVEF left ventricular ejection fraction; UA/NSTEMI unstable angina/non–ST-elevation myocardial infarction; UFH unfractionated heparin.<br />
3.2.3. Additional Management Considerations <strong>for</strong><br />
Antiplatelet and Anticoagulant Therapy<br />
CLASS I<br />
1. For UA/NSTEMI patients in whom an initial conservative strategy is<br />
selected and no subsequent features appear that would necessitate<br />
diagnostic angiography (recurrent symptoms/ischemia, HF, or<br />
serious arrhythmias), a stress test should be per<strong>for</strong>med. (Level of<br />
Evidence: B) (Fig. 8; Box O)<br />
a. If, after stress testing, <strong>the</strong> patient is classified as not at low risk,<br />
diagnostic angiography should be per<strong>for</strong>med. (Level of Evidence:<br />
A) (Fig. 8; Box E1)<br />
b. If, after stress testing, <strong>the</strong> patient is classified as being at low<br />
risk (Fig. 8; Box E2), <strong>the</strong> instructions noted below should be<br />
Downloaded from<br />
circ.ahajournals.org by on September 22, <strong>2007</strong><br />
followed in preparation <strong>for</strong> discharge (Fig. 8; Box K) (Level of<br />
Evidence: A):<br />
1. Continue ASA indefinitely. (Level of Evidence: A)<br />
2. Continue clopidogrel <strong>for</strong> at least 1 month (Level of Evidence:<br />
A) and ideally up to 1 year. (Level of Evidence: B)<br />
3. Discontinue intravenous GP IIb/IIIa inhibitor if started previously.<br />
(Level of Evidence: A)<br />
4. Continue UFH <strong>for</strong> 48 h or administer enoxaparin or fondaparinux<br />
<strong>for</strong> <strong>the</strong> duration of hospitalization, up to 8 d, and <strong>the</strong>n<br />
discontinue anticoagulant <strong>the</strong>rapy. (Level of Evidence: A)<br />
2. For UA/NSTEMI patients in whom CABG is selected as a postangiography<br />
management strategy, <strong>the</strong> instructions noted below<br />
should be followed (Fig. 9; Box G).













