Dr. Kloehn: Endokrinologie- NSD
Dr. Kloehn: Endokrinologie- NSD
Dr. Kloehn: Endokrinologie- NSD

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
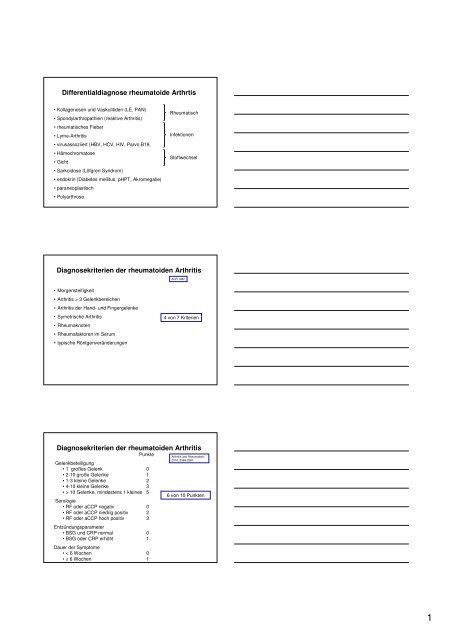
Differentialdiagnose rheumatoide Arthrtis<br />
• Kollagenosen und Vaskulitiden (LE, PAN)<br />
• Spondylarthropathien (reaktive Arthritis)<br />
• rheumatisches Fieber<br />
• Lyme-Arthritis<br />
• virusassoziiert (HBV, HCV, HIV, Parvo B19,<br />
• Hämochromatose<br />
• Gicht<br />
• Sarkoidose (Löfgren-Syndrom)<br />
• endokrin (Diabetes mellitus, pHPT, Akromegalie)<br />
• paraneoplastisch<br />
• Polyarthrose<br />
Rheumatisch<br />
Infektionen<br />
Stoffwechsel<br />
Diagnosekriterien der rheumatoiden Arthritis<br />
ACR 1987<br />
• Morgensteifigkeit<br />
• Arthritis > 3 Gelenkbereichen<br />
• Arthritis der Hand- und Fingergelenke<br />
• Symetrische Arthritis<br />
• Rheumaknoten<br />
• Rheumafaktoren im Serum<br />
• typische Röntgenveränderungen<br />
4 von 7 Kriterien<br />
Diagnosekriterien der rheumatoiden Arthritis<br />
Punkte<br />
Gelenkbeteiligung<br />
• 1 großes Gelenk 0<br />
• 2-10 große Gelenke 1<br />
• 1-3 kleine Gelenke 2<br />
• 4-10 kleine Gelenke 3<br />
• > 10 Gelenke, mindestens 1 kleines 5<br />
Serologie<br />
• RF oder aCCP negativ 0<br />
• RF oder aCCP niedrig positiv 2<br />
• RF oder aCCP hoch positiv 3<br />
Entzündungsparameter<br />
• BSG und CRP normal 0<br />
• BSG oder CRP erhöht 1<br />
Dauer der Symptome<br />
• < 6 Wochen 0<br />
• ≥ 6 Wochen 1<br />
Arthritis and Rheumatism;<br />
2010, 2569-2581<br />
6 von 10 Punkten<br />
1
Differential-Diagnose Hypercalcämie<br />
Phosphat Parathormon<br />
Besonderheit<br />
Tumorinduziert ⇔/⇑ ⇓ Mamma,Bronchial, Prostata, Plasmozytom<br />
Endokrin<br />
pHPT ⇓/⇔ ⇑<br />
Hyperthyreose ⇔ ⇓ ⇑ Knochenresorbtion<br />
M. Addison ⇔/⇑ ⇓ ⇑ enterale Ca-Absorbtion<br />
Medikamentös<br />
Vit D ⇔/⇑ ⇓<br />
Vit A, Thiazid ⇔ ⇓ ⇑ Knochenresorbtion, renale Reabsobtion<br />
Lithium ⇓/⇔ ⇑ Ca-Sensor-Rezeptor-Blockade<br />
Immobilisation ⇔ ⇓ v.a. junge Männer<br />
Sarkoidose ⇔/⇑ ⇓ ⇑ Vit-D-Bildung in Granulomen<br />
Familiäre<br />
hypocalciurische ⇔ ⇔/⇑ Ca-Sensor-Rezeptor-Defekt<br />
Hypercalcämie<br />
Skelett-Szintigraphie<br />
Früh<br />
rheumatoide<br />
Arthritis<br />
Spät<br />
Prüner Gang, Kiel<br />
S. <strong>Kloehn</strong><br />
21. Schilddrüsensymposium<br />
Kiel, 17.09.2011<br />
Halssonographie<br />
2
<strong>NSD</strong>-Szinti<br />
Nukleramedizin, Universitätsklinikum Kiel<br />
<strong>NSD</strong>-Szinti<br />
Nukleramedizin, Universitätsklinikum Kiel<br />
S. <strong>Kloehn</strong><br />
21. Schilddrüsensymposium<br />
Kiel, 17.09.2011<br />
Primärer Hyparparathyreoidismus<br />
Inzidenz:<br />
Geschichte:<br />
0,3% (3:1 Frauen:Männer)<br />
1880 Sandstrom: Erstbeschreibung Nebenschilddrüse<br />
1891 v. Recklinghausen: Osteitis fibrosis cystica<br />
∼1920 Erdheim: Hypercalcämie durch <strong>NSD</strong>-Hormon<br />
1934 Albright: „The case of Captian Charles Martell“<br />
„The patients [became] more and more skeletonless,<br />
more and more plant-like, until finally they were<br />
yellofish incapaple in lokomation, in same case dying<br />
of suffocation, unable to move the chest in<br />
respiration.“<br />
J clin Endocrinol Metab 1948<br />
Fuller Albright Collection,<br />
Massachuetts General Hospital<br />
3
Primärer Hyparparathyreoidismus<br />
The case of Captian Charles Martell<br />
1926<br />
J clin Endocrinol Metab 1948<br />
Primärer Hyparparathyreoidismus<br />
The case of Captian Charles Martell<br />
„The Captain ... lay in a ward<br />
slowly excreting skeleton into<br />
his urine“<br />
1926 1934<br />
J clin Endocrinol Metab 1948<br />
Primärer Hyparparathyreoidismus<br />
Häufigkeit: 20 % aller Hyperkalziämien<br />
Inzidenz: 4/100.000<br />
• 80-90 % Solitäres Adenom<br />
• Hyperplasie<br />
> MEN-1: Defekte des Menin-Gens<br />
> MEN-2: Mutation des Ret-protoonkogen<br />
> Hyperparathyreoidism-Jaw tumor Syndrome (HRPT2)<br />
• Nebenschilddrüsenkarzinom 1 %<br />
4
Die Chimäre im Körper:<br />
Primärer Hyparparathyreoidismus<br />
- Symptome -<br />
MEN I<br />
pHPT 95%<br />
Neuroendokrine Tumore 50%<br />
Hypophysentumore 25%<br />
Osteoporose/<br />
Frakturen<br />
Polyurie/Polydipsie<br />
Nephrolithiasis<br />
Knoten im<br />
Hals<br />
<strong>NSD</strong> ⇑<br />
pPTH ⇑<br />
Ca ⇑<br />
Schwäche<br />
MEN 2A<br />
medulläres SD-Ca 100%<br />
Phäochromozytom 50%<br />
pHPT 20%<br />
Knochenschmerzen<br />
Depression<br />
Dyspepsie/Ulcus<br />
primärer Hyperparathyreoidismus<br />
Diagnostik:<br />
•Labor: - Ca, Pho, AP, Albumin, Crea, Parathormon<br />
- Calzium im 24 h Urin<br />
•Sonographie<br />
•Chirurg<br />
•MIBI-Scan (bei Rezidiv/ Reoperation)<br />
Doppman JL 1991, Mitchell BK 1995, Weber CJ 1994<br />
• Operation: Indikation:<br />
• 0,25 mmol/l über der Norm<br />
• Regelmäßige Kontrollen nicht möglich<br />
Bilezikian JP; J Clin Endocrinol Metabol 2002<br />
5
Primärer Hyparparathyreoidismus<br />
- Therapie -<br />
Konservativ: Indikation<br />
• Asymptomatischer pHPT<br />
• Keine Symptome<br />
• OP abgelehnt<br />
• OP Kontraindikation<br />
→ reichlich Flüssigkeit<br />
→ Calziumaufnahme einschränken (
Klinik:<br />
Tetanisches Syndrom:<br />
Karpopedalspasmen, Parästhesien, Chvostek +,<br />
Troussaeu+, QT-Verlängerung, Krampfanfall<br />
Organmanifestation:<br />
Katarakt, Basalganglienverkalkung, Kardiomyopathie<br />
Weiterführende Untersuchungen:<br />
CT<br />
Hypoparathyreoidismus<br />
augenärztliche Untersuchung<br />
ggf. Echokardiographie<br />
Hypoparathyreoidismus<br />
Therapie:<br />
Akuter Anfall: 1 Ampulle 10% Ca-Lösung i.v., langsam;<br />
vor Gabe Blutentnahme!<br />
Digitalis!<br />
Langzeittherapie:<br />
Ziel: Calzium 2,0-2,2 mmol/l<br />
Gleichmäßiges Calziumangebot (500-1000 mg/d)<br />
Vitamin D Colecalciferol 20.000-100.000 IE<br />
Calcitriol 0,5-1,5 ug<br />
Phosphatarme Diät, Aluminiumhydroxid-Präparate<br />
Parathormon?<br />
7