

March/April - West Virginia State Medical Association
March/April - West Virginia State Medical Association
March/April - West Virginia State Medical Association

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Scientific Article |<br />
Congenital Absence of Inferior Vena Cava with<br />
Idiopathic Deep Vein Thrombosis in an Adult<br />
Deepak Hooda, MD, MPH<br />
Fellow, WVU Heart Institute, Morgantown<br />
Karthik Penumetsa, MD<br />
Resident, Department of Medicine, WVU, Morgantown<br />
Timothy Jackson, MD<br />
Section Chief, Associate Professor of Medicine (SOM),<br />
WVU, Morgantown<br />
Wissam Gharib, MD<br />
Associate Professor of Medicine (SOM), WVU Heart<br />
Institute, WVU, Morgantown<br />
Robert J. Beto, MD<br />
Associate Professor of Medicine (SOM), WVU Heart<br />
Institute,WVU, Morgantown,<br />
Bradford E. Warden, MD<br />
Program Director (Cardiology), Associate Professor of<br />
Medicine (SOM), WVU Heart Institute,WVU,<br />
Morgantown<br />
Acknowledgement: Masroor<br />
Abro MD, Fellow WVU Heart<br />
Institute, Morgantown WV.<br />
Corresponding Author: Deepak Hooda, MD MPH, 1<br />
stadium drive, WVU Hospitals, Morgantown WV 26506<br />
deepak.hooda@gmail.com.<br />
Introduction<br />
Deep vein thrombosis (DVT)<br />
is rare in younger patients, with<br />
a prevalence of 1:10,000. 1 In this<br />
patient population congenital<br />
absence of inferior vena cava<br />
(CAIVC) is an anomaly which<br />
has been recognized as a rare<br />
inherited risk factor for DVT. 2 Such<br />
patients are often asymptomatic<br />
and are diagnosed incidentally.<br />
In a young patient with a new DVT<br />
and no risk factors, it is important to<br />
consider congenital anomalies in the<br />
differential diagnoses. We describe<br />
a case of CAIVC and condition<br />
that is often underreported due<br />
to lack of diagnostic accuracy.<br />
except smoking noted gradual<br />
onset of lower back pain and<br />
bilateral lower limb swelling for<br />
the past four weeks. On arrival he<br />
was wheelchair bound. He had no<br />
family history of clotting disorders,<br />
congenital defects or autoimmune<br />
diseases. After admission he<br />
underwent extensive investigation<br />
including a hypercoagulopathy<br />
panel, prothrombinII gene<br />
mutation, Methylenetetrahydrofolate<br />
reductase(MTHFR) gene mutation,<br />
homocystein, factorV leiden<br />
mutation, Beta2 glycoprotein IgA/<br />
IgM, anticardiolipin IgG/IgM, lupus<br />
anticoagulant IgG/IgM, protein C&S<br />
antigen/functional levels, CD55&CD59<br />
antibodies and antithrombinIII<br />
antibodies. These tests were all<br />
negative. Subsequently a Doppler<br />
ultrasound of the lower limbs<br />
revealed extensive bilateral common<br />
femoral, superficial femoral,<br />
popliteal, posterior tibial and greater<br />
saphenous vein thromboses.<br />
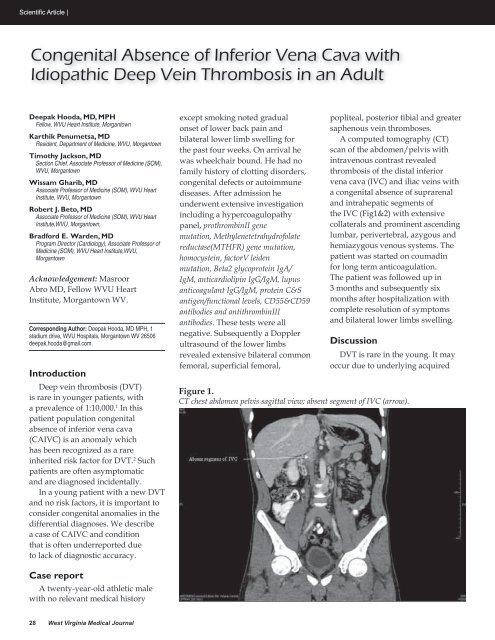
A computed tomography (CT)<br />
scan of the abdomen/pelvis with<br />
intravenous contrast revealed<br />
thrombosis of the distal inferior<br />
vena cava (IVC) and iliac veins with<br />
a congenital absence of suprarenal<br />
and intrahepatic segments of<br />
the IVC (Fig1&2) with extensive<br />
collaterals and prominent ascending<br />
lumbar, perivertebral, azygous and<br />
hemiazygous venous systems. The<br />
patient was started on coumadin<br />
for long term anticoagulation.<br />
The patient was followed up in<br />
3 months and subsequently six<br />
months after hospitalization with<br />
complete resolution of symptoms<br />
and bilateral lower limbs swelling.<br />
Discussion<br />
DVT is rare in the young. It may<br />
occur due to underlying acquired<br />
Figure 1.<br />
CT chest abdomen pelvis sagittal view: absent segment of IVC (arrow).<br />
Case report<br />
A twenty-year-old athletic male<br />
with no relevant medical history<br />
28 <strong>West</strong> <strong>Virginia</strong> <strong>Medical</strong> Journal












