

March/April - West Virginia State Medical Association
March/April - West Virginia State Medical Association
March/April - West Virginia State Medical Association

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Scientific Article |<br />
Obstructive Uropathy Secondary to Rectus<br />
Sheath Hematoma<br />
Pankaj P. Dangle, MD<br />
Saint Louis University School of Medicine, Department<br />
of Surgery, Division of Urology<br />
Mitesh B. Patel, MS III<br />
Saint Louis University School of Medicine<br />
Marcos Terán, MS, MS III<br />
Saint Louis University School of Medicine<br />
Micheal J. Chehval, MD<br />
Saint Louis University School of Medicine, Department<br />
of Surgery, Division of Urology<br />
Corresponding Author: Pankaj P. Dangle MD, Mch, 3517<br />
South Hoyne Ave Unit 6, Chicago Il 60609 pankajdangle@<br />
gmail.com<br />
Abbreviations: RSH – Rectus<br />
sheath hematoma, DVT – Deep<br />
vein thrombosis, PE – Pulmonary<br />
embolus, OSH – Outside<br />
hospital, INR – International<br />
normalized ratio, BUN – Blood<br />
urea nitrogen, Cr - Creatinine,<br />
CT – Computed tomography<br />
Abstract<br />
Rectus sheath hematoma (RSH) is<br />
uncommon and is often reported in the<br />
setting of anticoagulation or trauma.<br />
Typically RSH presents with localized or<br />
diffuse abdominal pain and a fixed<br />
abdominal wall mass, however, various<br />
presentations and complications have<br />
been reported depending on the setting<br />
and extent of the hematoma. We report a<br />
case of a rapidly expanding RSH causing<br />
obstructive anuria and hydronephrosis in<br />
addition to a review of literature on this<br />
rare presentation of RSH.<br />
Introduction<br />
Rectus sheath hematoma is<br />
a collection of blood within the<br />
abdominal wall musculature or<br />
fascia. RSH frequently presents<br />
with acute abdomen in the setting<br />
of anticoagulation or trauma, but<br />
various presentations have been<br />
reported. Symptoms can range from<br />
slight abdominal pain to hypovolemic<br />
shock. Although uncommon, RSH<br />
is important to consider in the<br />
differential for acute abdomen as<br />
a patient may clinically deteriorate<br />
and become hemodynamically<br />
unstable if bleeding persists. We<br />
report a case of a rapidly expanding<br />
RSH causing obstructive anuria<br />
and hydronephrosis in addition<br />
to a review of literature on this<br />
rare presentation of RSH.<br />
Case Report<br />
An obese 58-year-old woman on<br />
day ten of Coumadin therapy for<br />
deep vein thrombosis (DVT) and<br />
pulmonary embolus (PE) presented<br />
with an acute-onset of severe lower<br />
abdominal pain, nausea, and urge to<br />
void hours after a bout of coughing.<br />
Prior to transfer, exam at an outside<br />
hospital (OSH) demonstrated<br />
elevated blood pressure, tachycardia,<br />
diffuse abdominal tenderness,<br />
distension, and negative for a<br />
palpable mass. Laboratory evaluation<br />
showed an International Normalized<br />
ratio (INR) of 3.3, low hematocrit,<br />
and a blood urea nitrogen (BUN)<br />
and creatinine (Cr) of 25 and 2.1,<br />
respectively. She had minimal urine<br />
output with moderate blood and<br />
protein. CT scan with contrast of<br />
the abdomen and pelvis revealed<br />
a Grade 3 left rectus muscle<br />
hematoma contiguous into the pelvis,<br />
displacing the bladder superiorly<br />
and posteriorly to the right.<br />
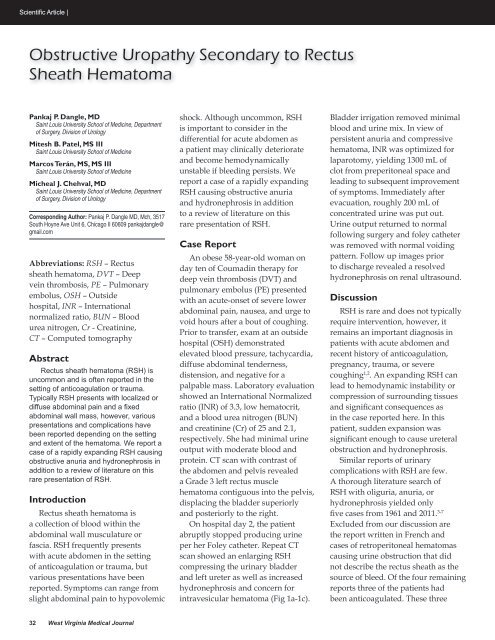
On hospital day 2, the patient<br />
abruptly stopped producing urine<br />
per her Foley catheter. Repeat CT<br />
scan showed an enlarging RSH<br />
compressing the urinary bladder<br />
and left ureter as well as increased<br />
hydronephrosis and concern for<br />
intravesicular hematoma (Fig 1a-1c).<br />
Bladder irrigation removed minimal<br />
blood and urine mix. In view of<br />
persistent anuria and compressive<br />
hematoma, INR was optimized for<br />
laparotomy, yielding 1300 mL of<br />
clot from preperitoneal space and<br />
leading to subsequent improvement<br />
of symptoms. Immediately after<br />
evacuation, roughly 200 mL of<br />
concentrated urine was put out.<br />
Urine output returned to normal<br />
following surgery and foley catheter<br />
was removed with normal voiding<br />
pattern. Follow up images prior<br />
to discharge revealed a resolved<br />
hydronephrosis on renal ultrasound.<br />
Discussion<br />
RSH is rare and does not typically<br />
require intervention, however, it<br />
remains an important diagnosis in<br />
patients with acute abdomen and<br />
recent history of anticoagulation,<br />
pregnancy, trauma, or severe<br />
coughing 1,2 . An expanding RSH can<br />
lead to hemodynamic instability or<br />
compression of surrounding tissues<br />
and significant consequences as<br />
in the case reported here. In this<br />
patient, sudden expansion was<br />
significant enough to cause ureteral<br />
obstruction and hydronephrosis.<br />
Similar reports of urinary<br />
complications with RSH are few.<br />
A thorough literature search of<br />
RSH with oliguria, anuria, or<br />
hydronephrosis yielded only<br />
five cases from 1961 and 2011. 3-7<br />
Excluded from our discussion are<br />
the report written in French and<br />
cases of retroperitoneal hematomas<br />
causing urine obstruction that did<br />
not describe the rectus sheath as the<br />
source of bleed. Of the four remaining<br />
reports three of the patients had<br />
been anticoagulated. These three<br />
32 <strong>West</strong> <strong>Virginia</strong> <strong>Medical</strong> Journal












