Provider Guide - the Culinary Health Fund
Provider Guide - the Culinary Health Fund
Provider Guide - the Culinary Health Fund

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
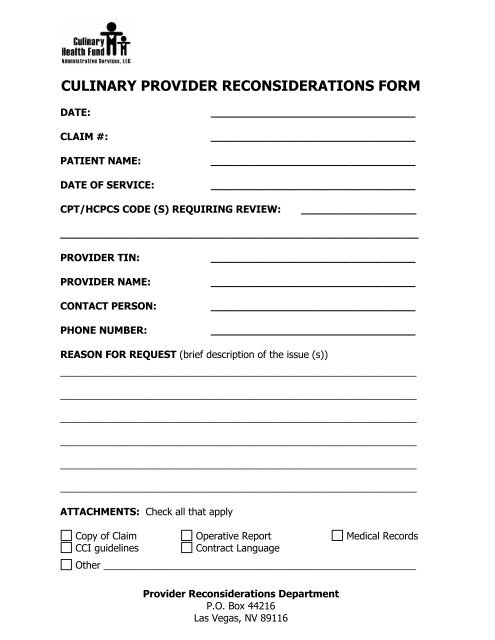
CULINARY PROVIDER RECONSIDERATIONS FORM<br />
DATE:<br />
CLAIM #:<br />
PATIENT NAME:<br />
DATE OF SERVICE:<br />
________________________________<br />
________________________________<br />
________________________________<br />
________________________________<br />
CPT/HCPCS CODE (S) REQUIRING REVIEW:<br />
__________________<br />
________________________________________________________<br />
PROVIDER TIN:<br />
PROVIDER NAME:<br />
CONTACT PERSON:<br />
PHONE NUMBER:<br />
________________________________<br />
________________________________<br />
________________________________<br />
________________________________<br />
REASON FOR REQUEST (brief description of <strong>the</strong> issue (s))<br />
_________________________________________________________________<br />
_________________________________________________________________<br />
_________________________________________________________________<br />
_________________________________________________________________<br />
_________________________________________________________________<br />
_________________________________________________________________<br />
ATTACHMENTS: Check all that apply<br />
Copy of Claim Operative Report Medical Records<br />
CCI guidelines<br />
Contract Language<br />
O<strong>the</strong>r _________________________________________________________<br />
<strong>Provider</strong> Reconsiderations Department<br />
P.O. Box 44216<br />
Las Vegas, NV 89116