Southern Adelaide Local Health Network - Falls Prevention in SA
Southern Adelaide Local Health Network - Falls Prevention in SA
Southern Adelaide Local Health Network - Falls Prevention in SA

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
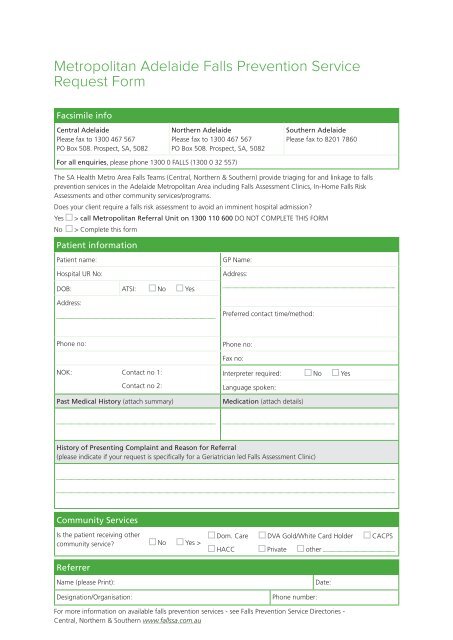
Metropolitan <strong>Adelaide</strong> <strong>Falls</strong> <strong>Prevention</strong> Service<br />
Request Form<br />
Facsimile <strong>in</strong>fo<br />
Central <strong>Adelaide</strong><br />
Please fax to 1300 467 567<br />
PO Box 508. Prospect, <strong>SA</strong>, 5082<br />
Northern <strong>Adelaide</strong><br />
Please fax to 1300 467 567<br />
PO Box 508. Prospect, <strong>SA</strong>, 5082<br />
<strong>Southern</strong> <strong>Adelaide</strong><br />
Please fax to 8201 7860<br />
For all enquiries, please phone 1300 0 FALLS (1300 0 32 557)<br />
The <strong>SA</strong> <strong>Health</strong> Metro Area <strong>Falls</strong> Teams (Central, Northern & <strong>Southern</strong>) provide triag<strong>in</strong>g for and l<strong>in</strong>kage to falls<br />
prevention services <strong>in</strong> the <strong>Adelaide</strong> Metropolitan Area <strong>in</strong>clud<strong>in</strong>g <strong>Falls</strong> Assessment Cl<strong>in</strong>ics, In-Home <strong>Falls</strong> Risk<br />
Assessments and other community services/programs.<br />
Does your client require a falls risk assessment to avoid an imm<strong>in</strong>ent hospital admission?<br />
Yes > call Metropolitan Referral Unit on 1300 110 600 DO NOT COMPLETE THIS FORM<br />
No > Complete this form<br />
Patient <strong>in</strong>formation<br />
Patient name:<br />
Hospital UR No:<br />
GP Name:<br />
Address:<br />
DOB: ATSI: No Yes<br />
Address:<br />
Preferred contact time/method:<br />
Phone no: Phone no:<br />
Fax no:<br />
NOK: Contact no 1:<br />
Contact no 2:<br />
Past Medical History (attach summary)<br />
Interpreter required: No Yes<br />
Language spoken:<br />
Medication (attach details)<br />
History of Present<strong>in</strong>g Compla<strong>in</strong>t and Reason for Referral<br />
(please <strong>in</strong>dicate if your request is specifically for a Geriatrician led <strong>Falls</strong> Assessment Cl<strong>in</strong>ic)<br />
Community Services<br />
Is the patient receiv<strong>in</strong>g other<br />
community service? No Yes ><br />
Dom. Care DVA Gold/White Card Holder CACPS<br />
HACC Private other<br />
Referrer<br />
Name (please Pr<strong>in</strong>t):<br />
Designation/Organisation:<br />
Phone number:<br />
Date:<br />
For more <strong>in</strong>formation on available falls prevention services - see <strong>Falls</strong> <strong>Prevention</strong> Service Directories -<br />
Central, Northern & <strong>Southern</strong> www.fallssa.com.au