Wound Closure Manual (PDF) - Penn Medicine
Wound Closure Manual (PDF) - Penn Medicine
Wound Closure Manual (PDF) - Penn Medicine

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
with absorbable suture material<br />
is usually preferred. Interrupted<br />
sutures can also be used for<br />
this procedure.<br />
FASCIA<br />
This layer of firm, strong connective<br />
tissue covering the muscles is the<br />
main supportive structure of the<br />
body. In closing an abdominal<br />
incision, the fascial sutures must<br />
hold the wound closed and<br />
also help to resist changes in intraabdominal<br />
pressure. Occasionally,<br />
synthetic graft material may be<br />
used when fascia is absent or weak.<br />
PROLENE* polypropylene mesh may<br />
be used to replace abdominal wall<br />
or repair hernias when a great deal<br />
of stress will be placed on the suture<br />
line during healing. Nonabsorbable<br />
sutures such as PROLENE suture<br />
may be used to suture the graft to<br />
the tissue.<br />
Fascia regains approximately 40%<br />
of its original strength in 2 months.<br />
It may take up to a year or longer to<br />
regain maximum strength. Full<br />
original strength is never regained.<br />
The anatomic location and type of<br />
abdominal incision will influence<br />
how may layers of fascia will be<br />
sutured. The posterior fascial layer<br />
is always closed. The anterior layer<br />
may be cut and may also require<br />
suturing. Mass closure techniques<br />
are becoming the most popular.<br />
Most suture materials have some<br />
inherent degree of elasticity. If not<br />
tied too tightly, the suture will<br />
"give" to accommodate postoperative<br />
swelling that occurs. Stainless<br />
steel sutures, if tied too tightly, will<br />
cut like a knife as the tissue swells<br />
or as tension is placed upon the<br />
suture line. Because of the slow<br />
healing time and because the fascial<br />
suture must bear the maximum<br />
stress of the wound, a moderate size<br />
nonabsorbable suture may be used.<br />
An absorbable suture with longer<br />
lasting tensile strength, such as<br />
PDS* II sutures, may also provide<br />
adequate support. PDS II sutures<br />
are especially well-suited for use in<br />
younger, healthy patients.<br />
Many surgeons prefer the use of<br />
interrupted simple or figure-of eight<br />
sutures to close fascia, while others<br />
employ running suture or a<br />
combination of these techniques.<br />
In the absence of infection or gross<br />
contamination, the surgeon may<br />
choose either monofilament or<br />
multifilament sutures. In the<br />
presence of infection, a<br />
CHAPTER 2 31<br />
monofilament absorbable material<br />
like PDS II sutures or inert nonabsorbable<br />
sutures like stainless steel or<br />
PROLENE* sutures may be used.<br />
MUSCLE<br />
Muscle does not tolerate suturing<br />
well. However, there are several<br />
options in this area.<br />
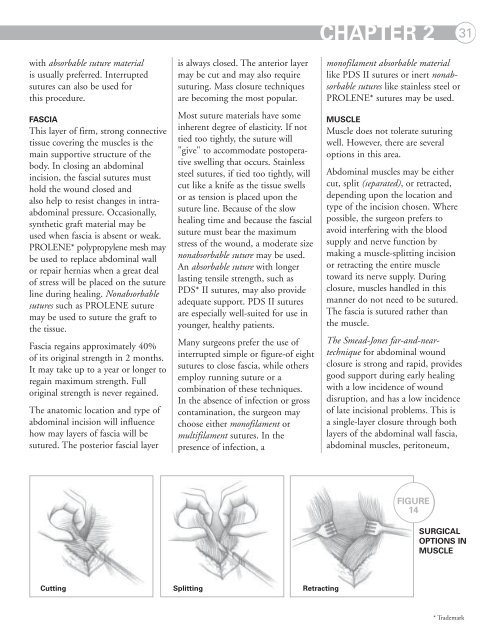
Abdominal muscles may be either<br />
cut, split (separated), or retracted,<br />
depending upon the location and<br />
type of the incision chosen. Where<br />
possible, the surgeon prefers to<br />
avoid interfering with the blood<br />
supply and nerve function by<br />
making a muscle-splitting incision<br />
or retracting the entire muscle<br />
toward its nerve supply. During<br />
closure, muscles handled in this<br />
manner do not need to be sutured.<br />
The fascia is sutured rather than<br />
the muscle.<br />
The Smead-Jones far-and-neartechnique<br />
for abdominal wound<br />
closure is strong and rapid, provides<br />
good support during early healing<br />
with a low incidence of wound<br />
disruption, and has a low incidence<br />
of late incisional problems. This is<br />
a single-layer closure through both<br />
layers of the abdominal wall fascia,<br />
abdominal muscles, peritoneum,<br />
FIGURE<br />
14<br />
SURGICAL<br />
OPTIONS IN<br />
MUSCLE<br />
Cutting Splitting Retracting<br />
* Trademark