

One-on-One An Interview with Dr. Paul Homoly Simply Beautiful A ...
One-on-One An Interview with Dr. Paul Homoly Simply Beautiful A ...
One-on-One An Interview with Dr. Paul Homoly Simply Beautiful A ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
In the normal osseous crest, the<br />
“<br />
facial margin of the preparati<strong>on</strong><br />
should be 2 mm to 2.5 mm<br />
cor<strong>on</strong>al to the osseous crest,<br />
or 0.5 mm to 1 mm apical to<br />
the free gingival margin.<br />
”<br />
surements, which should be of the entire dentogingival<br />
complex, will be the guide for placing the finish line of<br />
the preparati<strong>on</strong>.<br />
Ideally, for anterior teeth, the facial measurement should<br />
be approximately 3 mm, and the interproximal measurement,<br />
when adjacent teeth are present, approximately<br />
4 mm. This relati<strong>on</strong>ship is c<strong>on</strong>sidered a normal crest 6<br />
and exists <strong>on</strong> the facial and interproximal surfaces of<br />
normal sized teeth in about 85 percent of patients (Figure<br />
2). With this gingival-to-osseous crest relati<strong>on</strong>ship, if<br />
the tissue is traumatized <strong>with</strong> any type of clinical procedure,<br />
it will heal in a similar fashi<strong>on</strong>. 7 The healing will<br />
return to normal 85 percent of the time. 8<br />
If the depth of the osseous crest to the gingival margin<br />
is greater than 3 mm facially and 4 mm interproximally,<br />
it is c<strong>on</strong>sidered a low crest and exists <strong>on</strong> the facial and<br />
interproximal surfaces of normal sized teeth in about<br />
13 percent of patients. The low osseous crest and thin<br />
tissue biotype pose the most variati<strong>on</strong> for final gingival<br />
positi<strong>on</strong>. 9 Black holes and recessi<strong>on</strong> are most likely <strong>with</strong><br />
this situati<strong>on</strong>. If the gingival depth to the osseous crest<br />
is less than 3 mm facially and 4 mm interproximally, the<br />
osseous architecture is c<strong>on</strong>sidered a high crest and exists<br />
in about 2 percent of patients. High crests are most<br />
susceptible to biologic width violati<strong>on</strong>s.<br />
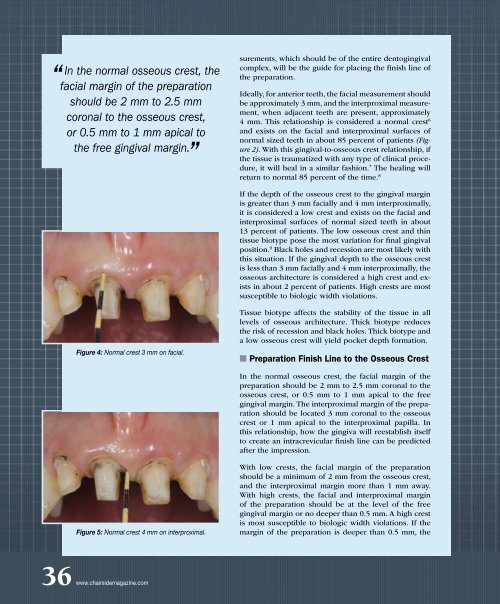
Figure 4: Normal crest 3 mm <strong>on</strong> facial.<br />
Tissue biotype affects the stability of the tissue in all<br />
levels of osseous architecture. Thick biotype reduces<br />
the risk of recessi<strong>on</strong> and black holes. Thick biotype and<br />
a low osseous crest will yield pocket depth formati<strong>on</strong>.<br />
■ Preparati<strong>on</strong> Finish Line to the Osseous Crest<br />
In the normal osseous crest, the facial margin of the<br />
preparati<strong>on</strong> should be 2 mm to 2.5 mm cor<strong>on</strong>al to the<br />
osseous crest, or 0.5 mm to 1 mm apical to the free<br />
gingival margin. The interproximal margin of the preparati<strong>on</strong><br />
should be located 3 mm cor<strong>on</strong>al to the osseous<br />
crest or 1 mm apical to the interproximal papilla. In<br />
this relati<strong>on</strong>ship, how the gingiva will reestablish itself<br />
to create an intracrevicular finish line can be predicted<br />
after the impressi<strong>on</strong>.<br />
Figure 5: Normal crest 4 mm <strong>on</strong> interproximal.<br />
With low crests, the facial margin of the preparati<strong>on</strong><br />
should be a minimum of 2 mm from the osseous crest,<br />
and the interproximal margin more than 1 mm away.<br />
With high crests, the facial and interproximal margin<br />
of the preparati<strong>on</strong> should be at the level of the free<br />
gingival margin or no deeper than 0.5 mm. A high crest<br />
is most susceptible to biologic width violati<strong>on</strong>s. If the<br />
margin of the preparati<strong>on</strong> is deeper than 0.5 mm, the<br />
36 www.chairsidemagazine.com














