professional/support staff leaves of absence without pay
professional/support staff leaves of absence without pay
professional/support staff leaves of absence without pay

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
G-2931 GCCC-EA<br />
EXHIBIT<br />
EXHIBIT<br />
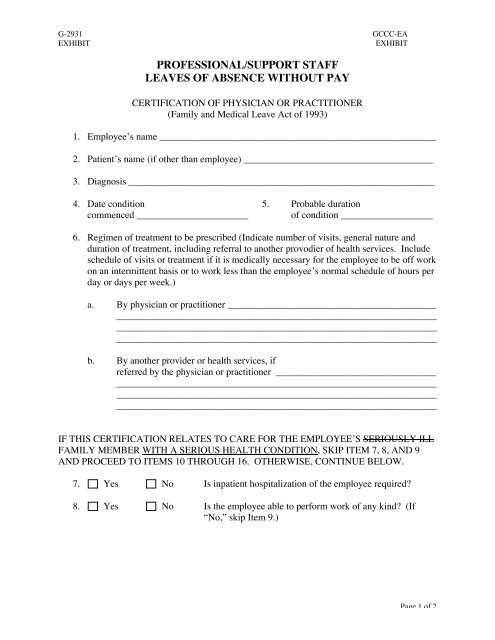
PROFESSIONAL/SUPPORT STAFF<br />
LEAVES OF ABSENCE WITHOUT PAY<br />
CERTIFICATION OF PHYSICIAN OR PRACTITIONER<br />
(Family and Medical Leave Act <strong>of</strong> 1993)<br />
1. Employee’s name _________________________________________________________<br />
2. Patient’s name (if other than employee) _______________________________________<br />
3. Diagnosis _______________________________________________________________<br />
4. Date condition 5. Probable duration<br />
commenced _______________________ <strong>of</strong> condition ___________________<br />
6. Regimen <strong>of</strong> treatment to be prescribed (Indicate number <strong>of</strong> visits, general nature and<br />
duration <strong>of</strong> treatment, including referral to another provodier <strong>of</strong> health services. Include<br />
schedule <strong>of</strong> visits or treatment if it is medically necessary for the employee to be <strong>of</strong>f work<br />
on an intermittent basis or to work less than the employee’s normal schedule <strong>of</strong> hours per<br />
day or days per week.)<br />
a. By physician or practitioner ___________________________________________<br />
__________________________________________________________________<br />
__________________________________________________________________<br />
__________________________________________________________________<br />
b. By another provider or health services, if<br />
referred by the physician or practitioner _________________________________<br />
__________________________________________________________________<br />
__________________________________________________________________<br />
__________________________________________________________________<br />
IF THIS CERTIFICATION RELATES TO CARE FOR THE EMPLOYEE’S SERIOUSLY ILL<br />
FAMILY MEMBER WITH A SERIOUS HEALTH CONDITION, SKIP ITEM 7, 8, AND 9<br />
AND PROCEED TO ITEMS 10 THROUGH 16. OTHERWISE, CONTINUE BELOW.<br />
7. Yes No Is inpatient hospitalization <strong>of</strong> the employee required?<br />
8. Yes No Is the employee able to perform work <strong>of</strong> any kind? (If<br />
“No,” skip Item 9.)<br />
Page 1 <strong>of</strong> 2
G-2931 GCCC-EA<br />
EXHIBIT<br />
EXHIBIT<br />
9. Yes No Is the employee able to perform the functions <strong>of</strong> the<br />
employee’s position? (Answer after reviewing a statement<br />
from the employer <strong>of</strong> essential functions <strong>of</strong> the employee’s<br />
position, or, if none is provided, after discussing it with the<br />
employee.)<br />
10. Yes No Is inpatient hospitalization <strong>of</strong> the family member (patient)<br />
required?<br />
11. Yes No Does (or will) the patient require assistance for basic<br />
medical, hygiene, nutritional needs, safety, or<br />
transportation?<br />
12. Yes No After review <strong>of</strong> the employee’s signed statement (see<br />
“Employee Statement” below), is the employee’s presence<br />
necessary, or would it be beneficial for the care <strong>of</strong> the<br />
patient?<br />
13. Estimate the period <strong>of</strong> time care is needed or<br />
the employee’s presence would be beneficial. __________________________________<br />
14. Signature <strong>of</strong> physician or practitioner _________________________________________<br />
15. Date ___________________________________________________________________<br />
16. Type <strong>of</strong> practice or field <strong>of</strong> specialty __________________________________________<br />
Employee Statement<br />
Complete the following when family leave is needed to care for a (seriously ill) family member<br />
with a serious health condition or to care for a servicemember.<br />
What care will the employee provide?_______________________________________________<br />
______________________________________________________________________________<br />
______________________________________________________________________________<br />
Estimate what the time period will be during which the employee will care for the family<br />
member. (If intermittent or reduced leave is anticipated, provide a suggested schedule.)<br />
______________________________________________________________________________<br />
______________________________________________________________________________<br />
______________________________________________________________________________<br />
_________________________________________<br />
Employee Signature<br />
______________________________<br />
Date<br />
Page 2 <strong>of</strong> 2