Member Handbook for Parkland KIDSfirst and Parkland CHIP ...
Member Handbook for Parkland KIDSfirst and Parkland CHIP ...
Member Handbook for Parkland KIDSfirst and Parkland CHIP ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
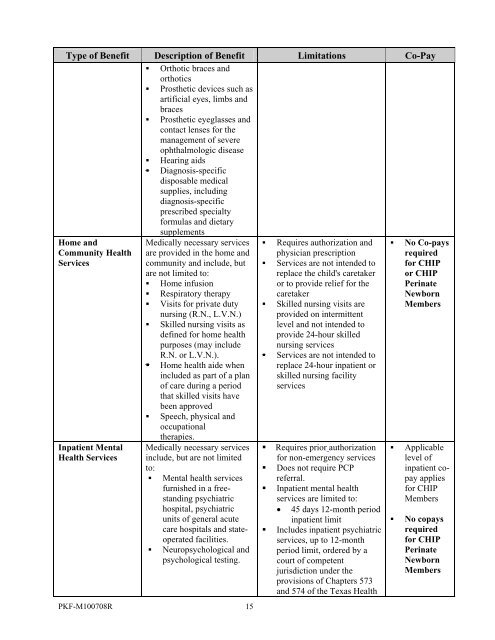
Type of Benefit Description of Benefit Limitations Co-Pay<br />
• Orthotic braces <strong>and</strong><br />
orthotics<br />
• Prosthetic devices such as<br />
artificial eyes, limbs <strong>and</strong><br />
braces<br />
• Prosthetic eyeglasses <strong>and</strong><br />
contact lenses <strong>for</strong> the<br />
management of severe<br />
ophthalmologic disease<br />
• Hearing aids<br />
• Diagnosis-specific<br />
disposable medical<br />
supplies, including<br />
diagnosis-specific<br />
prescribed specialty<br />
<strong>for</strong>mulas <strong>and</strong> dietary<br />
supplements<br />
Home <strong>and</strong><br />
Community Health<br />
Services<br />
Inpatient Mental<br />
Health Services<br />
Medically necessary services<br />
are provided in the home <strong>and</strong><br />
community <strong>and</strong> include, but<br />
are not limited to:<br />
• Home infusion<br />
• Respiratory therapy<br />
• Visits <strong>for</strong> private duty<br />
nursing (R.N., L.V.N.)<br />
• Skilled nursing visits as<br />
defined <strong>for</strong> home health<br />
purposes (may include<br />
R.N. or L.V.N.).<br />
• Home health aide when<br />
included as part of a plan<br />
of care during a period<br />
that skilled visits have<br />
been approved<br />
• Speech, physical <strong>and</strong><br />
occupational<br />
therapies.<br />
Medically necessary services<br />
include, but are not limited<br />
to:<br />
• Mental health services<br />
furnished in a freest<strong>and</strong>ing<br />
psychiatric<br />
hospital, psychiatric<br />
units of general acute<br />
care hospitals <strong>and</strong> stateoperated<br />
facilities.<br />
• Neuropsychological <strong>and</strong><br />
psychological testing.<br />
PKF-M100708R 15<br />
• Requires authorization <strong>and</strong><br />
physician prescription<br />
• Services are not intended to<br />
replace the child's caretaker<br />
or to provide relief <strong>for</strong> the<br />
caretaker<br />
• Skilled nursing visits are<br />
provided on intermittent<br />
level <strong>and</strong> not intended to<br />
provide 24-hour skilled<br />
nursing services<br />
• Services are not intended to<br />
replace 24-hour inpatient or<br />
skilled nursing facility<br />
services<br />
• Requires prior authorization<br />
<strong>for</strong> non-emergency services<br />
• Does not require PCP<br />
referral.<br />
• Inpatient mental health<br />
services are limited to:<br />
• 45 days 12-month period<br />
inpatient limit<br />
• Includes inpatient psychiatric<br />
services, up to 12-month<br />
period limit, ordered by a<br />
court of competent<br />
jurisdiction under the<br />
provisions of Chapters 573<br />
<strong>and</strong> 574 of the Texas Health<br />
• No Co-pays<br />
required<br />
<strong>for</strong> <strong>CHIP</strong><br />
or <strong>CHIP</strong><br />
Perinate<br />
Newborn<br />
<strong>Member</strong>s<br />
• Applicable<br />
level of<br />
inpatient copay<br />
applies<br />
<strong>for</strong> <strong>CHIP</strong><br />
<strong>Member</strong>s<br />
• No copays<br />
required<br />
<strong>for</strong> <strong>CHIP</strong><br />
Perinate<br />
Newborn<br />
<strong>Member</strong>s