doppler evaluation of valvular stenosis #3 - Echo in Context
doppler evaluation of valvular stenosis #3 - Echo in Context
doppler evaluation of valvular stenosis #3 - Echo in Context

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
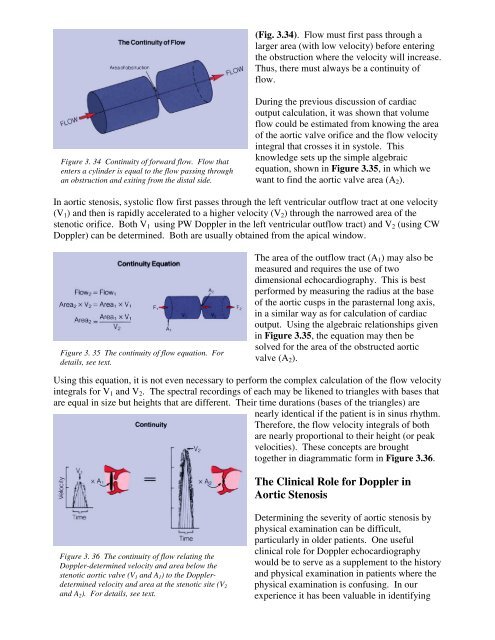
(Fig. 3.34). Flow must first pass through a<br />
larger area (with low velocity) before enter<strong>in</strong>g<br />
the obstruction where the velocity will <strong>in</strong>crease.<br />
Thus, there must always be a cont<strong>in</strong>uity <strong>of</strong><br />
flow.<br />
Figure 3. 34 Cont<strong>in</strong>uity <strong>of</strong> forward flow. Flow that<br />
enters a cyl<strong>in</strong>der is equal to the flow pass<strong>in</strong>g through<br />
an obstruction and exit<strong>in</strong>g from the distal side.<br />
Dur<strong>in</strong>g the previous discussion <strong>of</strong> cardiac<br />
output calculation, it was shown that volume<br />
flow could be estimated from know<strong>in</strong>g the area<br />
<strong>of</strong> the aortic valve orifice and the flow velocity<br />
<strong>in</strong>tegral that crosses it <strong>in</strong> systole. This<br />
knowledge sets up the simple algebraic<br />
equation, shown <strong>in</strong> Figure 3.35, <strong>in</strong> which we<br />
want to f<strong>in</strong>d the aortic valve area (A 2 ).<br />
In aortic <strong>stenosis</strong>, systolic flow first passes through the left ventricular outflow tract at one velocity<br />
(V 1 ) and then is rapidly accelerated to a higher velocity (V 2 ) through the narrowed area <strong>of</strong> the<br />
stenotic orifice. Both V 1 us<strong>in</strong>g PW Doppler <strong>in</strong> the left ventricular outflow tract) and V 2 (us<strong>in</strong>g CW<br />
Doppler) can be determ<strong>in</strong>ed. Both are usually obta<strong>in</strong>ed from the apical w<strong>in</strong>dow.<br />
Figure 3. 35 The cont<strong>in</strong>uity <strong>of</strong> flow equation. For<br />
details, see text.<br />
The area <strong>of</strong> the outflow tract (A 1 ) may also be<br />
measured and requires the use <strong>of</strong> two<br />
dimensional echocardiography. This is best<br />
performed by measur<strong>in</strong>g the radius at the base<br />
<strong>of</strong> the aortic cusps <strong>in</strong> the parasternal long axis,<br />
<strong>in</strong> a similar way as for calculation <strong>of</strong> cardiac<br />
output. Us<strong>in</strong>g the algebraic relationships given<br />
<strong>in</strong> Figure 3.35, the equation may then be<br />
solved for the area <strong>of</strong> the obstructed aortic<br />
valve (A 2 ).<br />
Us<strong>in</strong>g this equation, it is not even necessary to perform the complex calculation <strong>of</strong> the flow velocity<br />
<strong>in</strong>tegrals for V 1 and V 2 . The spectral record<strong>in</strong>gs <strong>of</strong> each may be likened to triangles with bases that<br />
are equal <strong>in</strong> size but heights that are different. Their time durations (bases <strong>of</strong> the triangles) are<br />
nearly identical if the patient is <strong>in</strong> s<strong>in</strong>us rhythm.<br />
Therefore, the flow velocity <strong>in</strong>tegrals <strong>of</strong> both<br />
are nearly proportional to their height (or peak<br />
velocities). These concepts are brought<br />
together <strong>in</strong> diagrammatic form <strong>in</strong> Figure 3.36.<br />
The Cl<strong>in</strong>ical Role for Doppler <strong>in</strong><br />
Aortic Stenosis<br />
Figure 3. 36 The cont<strong>in</strong>uity <strong>of</strong> flow relat<strong>in</strong>g the<br />
Doppler-determ<strong>in</strong>ed velocity and area below the<br />
stenotic aortic valve (V 1 and A 1 ) to the Dopplerdeterm<strong>in</strong>ed<br />
velocity and area at the stenotic site (V 2<br />
and A 2 ). For details, see text.<br />
Determ<strong>in</strong><strong>in</strong>g the severity <strong>of</strong> aortic <strong>stenosis</strong> by<br />
physical exam<strong>in</strong>ation can be difficult,<br />
particularly <strong>in</strong> older patients. One useful<br />
cl<strong>in</strong>ical role for Doppler echocardiography<br />
would be to serve as a supplement to the history<br />
and physical exam<strong>in</strong>ation <strong>in</strong> patients where the<br />
physical exam<strong>in</strong>ation is confus<strong>in</strong>g. In our<br />
experience it has been valuable <strong>in</strong> identify<strong>in</strong>g