Dauzat 1997Dauzat M, Laroche JP, Deklunder G, Ayoub, J, Quére I, Lopez FM,Janbon C. Diagnosis of acute lower limb deep venous thrombosiswith ultrasound: trends ans controversies. J Cl<strong>in</strong> Ultrasound 1997;25(7):343–58. 97426095.Haas 1999Haas SK, Wolf H, Encke A, Fareed J. Prevention of fatal pulmonaryembolism by low molecular weight hepar<strong>in</strong> - a double bl<strong>in</strong>d comparisonof certopar<strong>in</strong> <strong>and</strong> unfractionated hepar<strong>in</strong>. Thromb HaemostasAugust 1999;Supplement:491.Jørgensen 1993Jorgensen LN, Wille-Jorgensen P, Hauch O. Prophylaxis of postoperativethrom boembolism with low molecular weight hepar<strong>in</strong>s. Br JSurg 1993;80:689–704. 93321028.Kjaergaard 1985Kjaergaard J, Esbensen K, Wille Jorgensen P, Jorgensen T, Thorup J,Bern<strong>in</strong>g H, Wold S. A multivariate pattern recognition study of riskfactors<strong>in</strong>dicat<strong>in</strong>g postoperative thromboembolism despite low-dosehepar<strong>in</strong> <strong>in</strong> major abdom<strong>in</strong>al surgery. Thromb Haemost 1985;54(2):409–12. 86097628.Leizorovicz 1997Leizorovicz A, Haugh MC. Low Molecular weight hepar<strong>in</strong><strong>in</strong> preventionof perioperative thrombosis (Protocol). In: Fowkes FGR, JanzonL, Kleijnen J, leng CG (eds.) Pripheral Vascular Diseases Moduleon The Cochrane Database of Systematic Reviews, (updated August1997). Available <strong>in</strong> The Cochrane Library (database on CDROM).The Cochrane Collaboration; Issue 4. Ox<strong>for</strong>d: Update Software;1997. In: Cochrane Library, 3, 2000. Ox<strong>for</strong>d: Update Software.Leizorovicz 1992Leizorovicz A, Haugh MC, Chapuis FR, Samama MM, BoisselJP. Low molecular weight hepapr<strong>in</strong> <strong>in</strong> prevention of perioperativethrombosis. Brit Med J 1992;305:913–20. 93091577.Mantoni 1997Mantoni M, Str<strong>and</strong>berg C, Neergaard K, Sloth C, Jørgensen PS,Thamsen H, Tørholm C, Paaske BP, Rasmussen SW, ChristensenSW, Wille-Jørgensen P. Triplex US <strong>in</strong> the diagnosis of asymptomaticdeep venous thrombosis. Acta Radiol 1997;38(2):327–31.97247030.Nurmohammed 1992Nurmohamed MT, Rosendaal FR, Buller HR, et al. Low molecularweight hepar<strong>in</strong> versus st<strong>and</strong>ard hepar<strong>in</strong> <strong>in</strong> general <strong>and</strong> orthopaedicsurgery: a meta-analysis. Lancet 1992;340:152–56. 92326472.Siragusa 1997Siragusa S, Beltrametti C, Barone M, Piovella F. Cl<strong>in</strong>ical course <strong>and</strong><strong>in</strong>cidence of post-thrombophlebitic syndrome after profound asymptomaticdeep ve<strong>in</strong> thrombosis. M<strong>in</strong>erva Cardioangiol 1997;45:57–66.Wille-Jorgensen 1991Wille-Jørgensen, P. Prophylaxis of postoperative thromboembolism.Danish Medical Bullet<strong>in</strong> 1991;38:203–28.Wille-Jørgensen 1988Wille-Jørgensen P, Kjaergaard J, Jørgensen T, Korsgaard Larsen T.Failure <strong>in</strong> prophylactic management of thromboembolic disease <strong>in</strong>colorectal surgery. Dis Colon Rectum 1988;31:384–6. 1988211380.Wille-Jørgensen 1990Wille-Jorgensen P, Ott P. Predict<strong>in</strong>g failure of low.dose prophylactichepar<strong>in</strong> <strong>in</strong> general surgical patients. Surg Gynecol Obstet 1990;171:126–30.Wille-Jørgensen 1992Wille-Jørgensen P, Jørgensen LN, Hauch O, Borris LC, Lassen MR,Nehen AM, Kjær L, Jensen R. Potential <strong>in</strong>fluence of observer variationon thromboprophylactic studies. Hæmostasis 1992;22:211–5.∗ Indicates the major publication <strong>for</strong> the studyT A B L E SCharacteristics of <strong>in</strong>cluded studiesStudy Butson 1981MethodsParticipantsInterventionsOutcomesRCT. Sealed envelopes. Not bl<strong>in</strong>ded. (Controlgroup = no treatment). No primary stratification of colorectalpatients.Elective general surgery patients. 119 r<strong>and</strong>omized. Non excluded. Leav<strong>in</strong>g 119 patients <strong>in</strong> per protocolanalysis as well as <strong>in</strong> <strong>in</strong>tention to treat analysis. Subgroup of 24 colorectal patients were distributed withrespectively 63 % <strong>and</strong> 37 % <strong>in</strong> the two treatment arms.Intermittent compression: Intermittent compression peroperatively <strong>and</strong> untill ambulant. Most of the patients24 to 48 hours postoperatively.Control: No treatment.Thromboembolic events: DVTBleed<strong>in</strong>g events: Not described.Diagnosis: radiofibr<strong>in</strong>ogen uptake test every day up to 14 days postoperatively or untill discharge. If positivetest then confirmed with venography.<strong>Hepar<strong>in</strong>s</strong> <strong>and</strong> <strong>mechanical</strong> <strong>methods</strong> <strong>for</strong> <strong>thromboprophylaxis</strong> <strong>in</strong> colorectal surgery (Review)Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd11
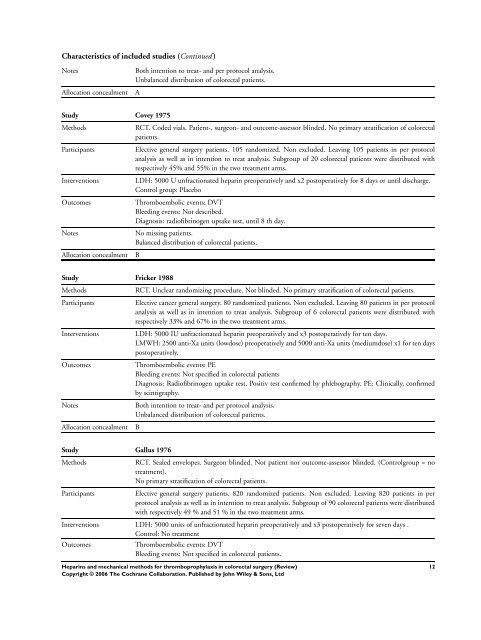
Characteristics of <strong>in</strong>cluded studies (Cont<strong>in</strong>ued )NotesAllocation concealmentBoth <strong>in</strong>tention to treat- <strong>and</strong> per protocol analysis.Unbalanced distribution of colorectal patients.AStudy Covey 1975MethodsParticipantsInterventionsOutcomesNotesAllocation concealmentRCT. Coded vials. Patient-, surgeon- <strong>and</strong> outcome-assessor bl<strong>in</strong>ded. No primary stratification of colorectalpatients.Elective general surgery patients. 105 r<strong>and</strong>omized. Non excluded. Leav<strong>in</strong>g 105 patients <strong>in</strong> per protocolanalysis as well as <strong>in</strong> <strong>in</strong>tention to treat analysis. Subgroup of 20 colorectal patients were distributed withrespectively 45% <strong>and</strong> 55% <strong>in</strong> the two treatment arms.LDH: 5000 U unfractionated hepar<strong>in</strong> preoperatively <strong>and</strong> x2 postoperatively <strong>for</strong> 8 days or until discharge.Control group: PlaceboThromboembolic events: DVTBleed<strong>in</strong>g events: Not described.Diagnosis: radiofibr<strong>in</strong>ogen uptake test, until 8 th day.No miss<strong>in</strong>g patients.Balanced distribution of colorectal patients.BStudy Fricker 1988MethodsParticipantsInterventionsOutcomesNotesAllocation concealmentRCT. Unclear r<strong>and</strong>omiz<strong>in</strong>g procedure. Not bl<strong>in</strong>ded. No primary stratification of colorectal patients.Elective cancer general surgery. 80 r<strong>and</strong>omized patients. Non excluded. Leav<strong>in</strong>g 80 patients <strong>in</strong> per protocolanalysis as well as <strong>in</strong> <strong>in</strong>tention to treat analysis. Subgroup of 6 colorectal patients were distributed withrespectively 33% <strong>and</strong> 67% <strong>in</strong> the two treatment arms.LDH: 5000 IU unfractionated hepar<strong>in</strong> preoperatively <strong>and</strong> x3 postoperatively <strong>for</strong> ten days.LMWH: 2500 anti-Xa units (lowdose) preoperatively <strong>and</strong> 5000 anti-Xa units (mediumdose) x1 <strong>for</strong> ten dayspostoperatively.Thromboembolic events: PEBleed<strong>in</strong>g events: Not specified <strong>in</strong> colorectal patientsDiagnosis: Radiofibr<strong>in</strong>ogen uptake test. Positiv test confirmed by phlebography. PE: Cl<strong>in</strong>ically, confirmedby sc<strong>in</strong>tigraphy.Both <strong>in</strong>tention to treat- <strong>and</strong> per protocol analysis.Unbalanced distribution of colorectal patients.BStudy Gallus 1976MethodsParticipantsRCT. Sealed envelopes. Surgeon bl<strong>in</strong>ded. Not patient nor outcome-assessor bl<strong>in</strong>ded. (Controlgroup = notreatment).No primary stratification of colorectal patients.Elective general surgery patients. 820 r<strong>and</strong>omized patients. Non excluded. Leav<strong>in</strong>g 820 patients <strong>in</strong> perprotocol analysis as well as <strong>in</strong> <strong>in</strong>tention to treat analysis. Subgroup of 90 colorectal patients were distributedwith respectively 49 % <strong>and</strong> 51 % <strong>in</strong> the two treatment arms.Interventions LDH: 5000 units of unfractionated hepar<strong>in</strong> preoperatively <strong>and</strong> x3 postoperatively <strong>for</strong> seven days .Control: No treatmentOutcomesThromboembolic events: DVTBleed<strong>in</strong>g events: Not specified <strong>in</strong> colorectal patients.<strong>Hepar<strong>in</strong>s</strong> <strong>and</strong> <strong>mechanical</strong> <strong>methods</strong> <strong>for</strong> <strong>thromboprophylaxis</strong> <strong>in</strong> colorectal surgery (Review)Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd12