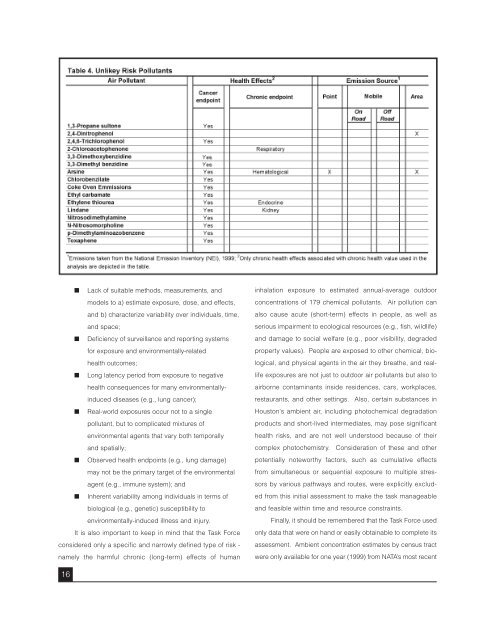
■ Lack of suitable methods, measurements, andmodels to a) estim<strong>at</strong>e exposure, dose, and effects,and b) characterize variability over <strong>in</strong>dividuals, time,and space;■ Deficiency of surveillance and report<strong>in</strong>g systemsfor exposure and environmentally-rel<strong>at</strong>edhealth outcomes;■ Long l<strong>at</strong>ency period from exposure to neg<strong>at</strong>ivehealth consequences for many environmentally<strong>in</strong>duceddiseases (e.g., lung cancer);■ Real-world exposures occur not to a s<strong>in</strong>glepollutant, but to complic<strong>at</strong>ed mixtures ofenvironmental agents th<strong>at</strong> vary both temporallyand sp<strong>at</strong>ially;■ Observed health endpo<strong>in</strong>ts (e.g., lung damage)may not be the primary target of the environmentalagent (e.g., immune system); and■ Inherent variability among <strong>in</strong>dividuals <strong>in</strong> terms ofbiological (e.g., genetic) susceptibility toenvironmentally-<strong>in</strong>duced illness and <strong>in</strong>jury.It is also important to keep <strong>in</strong> m<strong>in</strong>d th<strong>at</strong> the Task Forceconsidered only a specific and narrowly def<strong>in</strong>ed type of risk -namely the harmful chronic (long-term) effects of human<strong>in</strong>hal<strong>at</strong>ion exposure to estim<strong>at</strong>ed annual-average outdoorconcentr<strong>at</strong>ions of 179 chemical pollutants. <strong>Air</strong> pollution canalso cause acute (short-term) effects <strong>in</strong> people, as well asserious impairment to ecological resources (e.g., fish, wildlife)and damage to social welfare (e.g., poor visibility, degradedproperty values). People are exposed to other chemical, biological,and physical agents <strong>in</strong> the air they bre<strong>at</strong>he, and reallifeexposures are not just to outdoor air pollutants but also toairborne contam<strong>in</strong>ants <strong>in</strong>side residences, cars, workplaces,restaurants, and other sett<strong>in</strong>gs. Also, certa<strong>in</strong> substances <strong>in</strong><strong>Houston</strong>'s ambient air, <strong>in</strong>clud<strong>in</strong>g photochemical degrad<strong>at</strong>ionproducts and short-lived <strong>in</strong>termedi<strong>at</strong>es, may pose significanthealth risks, and are not well understood because of theircomplex photochemistry. Consider<strong>at</strong>ion of these and otherpotentially noteworthy factors, such as cumul<strong>at</strong>ive effectsfrom simultaneous or sequential exposure to multiple stressorsby various p<strong>at</strong>hways and routes, were explicitly excludedfrom this <strong>in</strong>itial assessment to make the task manageableand feasible with<strong>in</strong> time and resource constra<strong>in</strong>ts.F<strong>in</strong>ally, it should be remembered th<strong>at</strong> the Task Force usedonly d<strong>at</strong>a th<strong>at</strong> were on hand or easily obta<strong>in</strong>able to complete itsassessment. Ambient concentr<strong>at</strong>ion estim<strong>at</strong>es by census tractwere only available for one year (1999) from NATA’s most recent16
assessments, and monitor<strong>in</strong>g d<strong>at</strong>a from 20 st<strong>at</strong>ions <strong>in</strong> <strong>Houston</strong>were only available for a small fraction of HAPs, and only analyzed<strong>in</strong> depth for 2004, the most recent complete year. TheTask Force used “off-the-shelf” health values (UREs andRfCs/RELs/MRLs) from the U.S. EPA (U.S. EPA, 2005, 2006h,2006i), the California OEHHA (California EPA & OEHHA, 2002;California OEHHA, 2005) and the Agency for Toxic Substancesand Disease Registry (ATSDR) to estim<strong>at</strong>e health risks, implicitlyassum<strong>in</strong>g th<strong>at</strong> these unmodified risk values were uniformlyapplicable to the <strong>Houston</strong> situ<strong>at</strong>ion and popul<strong>at</strong>ion.SUMMARY OF AIR POLLUTION-RELATEDHEALTH EFFECTSThousands of epidemiologic (human) and toxicologic(animal) studies conducted over the past 35 years have documentedthe fact th<strong>at</strong> urban air pollution <strong>at</strong> sufficiently elev<strong>at</strong>edconcentr<strong>at</strong>ions can adversely affect human health. Poor airquality can potentially cause or contribute to a variety of harmfuloutcomes, rang<strong>in</strong>g from subtle biochemical and physiologicalchanges, to symptoms like headaches, eye and thro<strong>at</strong> irrit<strong>at</strong>ion,wheez<strong>in</strong>g and cough<strong>in</strong>g, difficulty bre<strong>at</strong>h<strong>in</strong>g, aggrav<strong>at</strong>ionof exist<strong>in</strong>g respir<strong>at</strong>ory and cardiovascular conditions,chronic respir<strong>at</strong>ory disease, cancer, and prem<strong>at</strong>ure de<strong>at</strong>h.Although the most obvious effects are typically on the respir<strong>at</strong>oryand cardiovascular systems, many air pollutants can harmdevelopment processes and be toxic to other systems, <strong>in</strong>clud<strong>in</strong>g,among others, nervous, reproductive, immune, digestive,ur<strong>in</strong>ary and endocr<strong>in</strong>e systems. In addition, numerous air pollutantsare known or suspected human carc<strong>in</strong>ogens.Ozone-rel<strong>at</strong>ed health effects are of special <strong>in</strong>terestbecause <strong>Houston</strong> currently exceeds the NAAQS standard.Ozone is a strong oxidiz<strong>in</strong>g agent, and short-term exposures onthe order of m<strong>in</strong>utes to hours can impair pulmonary function,decrease lung volumes and flows, and <strong>in</strong>crease airway responsiveness,resistance, and irrit<strong>at</strong>ion. Evidence <strong>in</strong>dic<strong>at</strong>es th<strong>at</strong> asubstantial fraction of summertime hospital visits and admissionsfor respir<strong>at</strong>ory problems are associ<strong>at</strong>ed with elev<strong>at</strong>edshort-term ozone levels. Repe<strong>at</strong>ed daily short-term exposure toozone can cause an <strong>in</strong>creased response to bronchial allergenchallenges <strong>in</strong> subjects with preexist<strong>in</strong>g allergic airway disease,with or without asthma. Long-term exposure to ozone overmonths to years can cause structural changes <strong>in</strong> the respir<strong>at</strong>orytract, and may play a role <strong>in</strong> caus<strong>in</strong>g irreversible lung damage.Ozone exposure can also impair the immune system soth<strong>at</strong> people are more susceptible to respir<strong>at</strong>ory <strong>in</strong>fections, likecolds and pneumonia.Although <strong>Houston</strong> does not exceed the current NAAQSfor either of the regul<strong>at</strong>ed fractions of particul<strong>at</strong>e m<strong>at</strong>ter (PM 2.5and PM 10), it is likely to exceed the new f<strong>in</strong>e (PM 2.5) particlestandard if and when it is promulg<strong>at</strong>ed. Particul<strong>at</strong>e m<strong>at</strong>ter is acomb<strong>in</strong><strong>at</strong>ion of solid, liquid, and solid-liquid particles suspended<strong>in</strong> air, and typically is composed of a complex mixture oforganic and <strong>in</strong>organic constituents. F<strong>in</strong>e particles, with aerodynamicdiameters ≤ 2.5 microns, are taken <strong>in</strong>to the deepest partof the lungs, where they tend to rema<strong>in</strong> trapped among millionsof t<strong>in</strong>y alveoli. Short-term exposures (m<strong>in</strong>utes to hours) to elev<strong>at</strong>edlevels of PM 2.5 have been l<strong>in</strong>ked with physiologicalchanges, biomarkers of cardiac changes, decreased lungfunction, <strong>in</strong>creased respir<strong>at</strong>ory symptoms, emergency roomvisits and hospitaliz<strong>at</strong>ion for cardiopulmonary diseases, andmortality from cardiopulmonary diseases. Longer-term exposures(months to years) have been causally associ<strong>at</strong>ed witheffects on the respir<strong>at</strong>ory system, such as decreased lung function,development of chronic respir<strong>at</strong>ory disease, and mortalityfrom cardiopulmonary diseases and lung cancer.There is no NAAQS for diesel particul<strong>at</strong>e m<strong>at</strong>ter, however,concerns about human health effects recently promptedCalifornia to list it as a Toxic <strong>Air</strong> Contam<strong>in</strong>ant (TAC) (CaliforniaARB, 1998; California ARB & OEHHA, 1998). Diesel exhaust,which is ubiquitous <strong>in</strong> urban environments, is a complex mixtureof hundreds of toxic substances, <strong>in</strong>clud<strong>in</strong>g gaseous andparticul<strong>at</strong>e constituents. The particles <strong>in</strong> diesel exhaust aremostly 2.5 microns, and are composed of an elemental carboncore with adsorbed organic compounds and small amounts ofsulf<strong>at</strong>e, nitr<strong>at</strong>e, metals, and other trace elements. Short-termexposures (m<strong>in</strong>utes to hours) may cause eye, thro<strong>at</strong>, andbronchial irrit<strong>at</strong>ion, lightheadedness, nausea, cough, andphlegm, as well as exacerb<strong>at</strong>ion of allergic responses andasthma-like symptoms. Long-term exposures (months toyears) may play a role <strong>in</strong> chronic respir<strong>at</strong>ory disease, and arelikely to <strong>in</strong>crease the risk of develop<strong>in</strong>g lung cancer.Short-term, high-level exposure (m<strong>in</strong>utes to hours) tomany of these substances, like benzene, toluene, and17
- Page 1 and 2: A Closer Look at Air Pollution in H
- Page 3 and 4: A Closer Look at Air Pollution in H
- Page 5 and 6: Task Force MembersResearch StaffKen
- Page 7 and 8: AcknowledgementsThe Task Force woul
- Page 10: Just because a task is difficult, h
- Page 13 and 14: ing, and route of exposure, and oth
- Page 15 and 16: and vulnerable subgroups. Substance
- Page 17: accurately from death certificates.
- Page 21 and 22: The reality is that, even at simila
- Page 23 and 24: ability, have inadequate means to c
- Page 25 and 26: Houston reaches $21,701. These are
- Page 27 and 28: In summary, we view the comparative
- Page 29 and 30: AppendicesPhoto by Heidi Bethel27
- Page 31 and 32: Photo by Heidi Bethelgrouping to a
- Page 33 and 34: Appendix 2the time period is repres
- Page 35 and 36: Appendix 3an appreciable risk of ad
- Page 37 and 38: Table A3.1. Health Values and Refer
- Page 39 and 40: Table A3.1. Health Values and Refer
- Page 41 and 42: Table A3.1. Health Values and Refer
- Page 43 and 44: Appendix 4Metals, Diesel PM Convers
- Page 45 and 46: Under advice from staff at the U.S.
- Page 47 and 48: Appendix 5Table A5.1. Uncertain Ris
- Page 49 and 50: Appendix 6Brief Descriptions of Hea
- Page 51 and 52: Appendix 7Summary Map and Table for
- Page 53 and 54: Appendix 8: Table 1Supplemental Tab
- Page 55 and 56: Appendix 8: Table 3Table A8.3. Poss
- Page 57 and 58: ReferencesHackett, P., Sikov, M., &