Review Articleincreased when unilateral or bilateral support ismissing 11 .Shortened dental arch may be associated withgreater tooth migration and interdental spacing,although migration was deemed small and clinicallyinsignificant. An SDA may also be associated withgreater over eruption of teeth. People with SDAshave been found to have more mobile teeth and loweralveolar bone levels. The combinations of increasedocclusal loading and existing periodontal diseaserepresent a risk factor for further loss of teeth in thosepeople. Patient with SDA probably also represent ahigh risk group in term of periodontal disease 12 .Oocclusal and TMJ Loads inShortened Dental Arches 13To determine whether shortened dental arches(SDAs) cause functional over loading of theteeth and the temporomandibular joint, whichhas been implicated in periodontal diseases andtemporomandibular disorders, the influences ofSDA on occlusal and joint loads were investigated.The finding of the studies provide no evidence thatshortened dental arch causes overloading of the teethand the joints, which suggests that neuromuscularregulatory system are controlling maximumclenching strength under various occlusal conditions.A possible explanation for these findings which denya relation between temporomandibular disorderand shortened dental arch is that neuromuscularregulatory mechanisms protect the joints fromoverloading. Because the sensory innervationsof this joint is limited mainly to the joint capsule,retrodiscal area and the posterior band of disk, neitherthe mechanoreceptors nor the nocireceptors in thejoint are well suited for detecting excessive loadduring clenching. The neuromuscular regulatorysystem thus seems designed to control the clenchingstrength so as not to exceed the critical limit of theload bearing capacity of periodontal tissues.ConclusionThe Shortened dental arch concept does notcontradict current occlusion theories and appears tofit well with the problem solving approach. It offerssome important advantages one of which is decreaseemphasis on restorative treatments for the posteriorregions of mouth. However, functional demands, andthe number of teeth to satisfy such demands varyfrom individual to individual hence they should betreated according to each individual need and adaptivecapability. SDA may avoid risk of overtreatment ofthe patient while still providing a high standard of careand minimizing cost. It may therefore be concludedthat this concepts deserves serious consideration intreatment planning for partially edentulous patients.However, ongoing changes in dental health andeconomy, the concept require continuing research,evaluation and discussion.References1. Van der Bilt A, Olthoff LW, Bosman F, Oosterhaven SP. Theeffect of missing postcanine teeth on chewing performancein man. Archives of Oral Biology 1993; 38: 423-9.2. Rodriguez AM, Aquilino SA, Lund PS. Cantilever andimplant biomechanics: a review of the literature, Part 2.Journal of Prosthodontics 1994; 3: 114-8.3. Kayser AF. Shortened dental arches and oral function.Journal of Oral Rehabilitation 1981; 8: 457 – 62.4. Kayser AF. Limited treatment goals- shortened dentalarches. Periodontology 2000 1994; 4:7- 14.5. Sarita PT, Witter DJ, Kreulen CM, Van’t Hof MA,Creugers NH. Chewing ability of subjects with shorteneddental arches. Community Dentistry Oral Epidemiology2003; 31: 328-34.6. Kanno T, Carlsson GE. A review of the shortened dentalarch concept focusing on the work by the Kayser/Nijmegen group. Journal of Oral Rehabilitation 2006;33(11): 850–62.7. Rosenoer LM, Sheiham A. Dental impacts on daily lifeand satisfaction with teeth in relation to dental status inadults. Journal of Oral Rehabilitation 1995; 7: 4469-80.8. Debora Armellini, J Anthony Von Fraunhofer. Theshortened dental arch: A review of literature. Journal ofProsthetic Dentistry 2004; 531-5.9. Witter DJ, N.H.J. Creugers, C.M. Kreulen. A.F.J. deHaan. Occlusal Stability in Shortened Dental Arches.Journal of Dental Research 2001; 80: 432-6.10. Witter DJ, Van Elteren P, Kayser AF, Van Rossum GM.Oral comfort in shortened dental arches. Journal of OralRehabilitation 1990; 17: 137-43.11. Witter DJ, Van Elteren P, Kayser AF, Van Rossum GM.Oral comfort in shortened dental arches. Journal of OralRehabilitation 1990; 17: 137-43.12. Witter DJ, van Elteren P, Kayser AF. Migration of teethin shortened dental arches. Journal of Oral Rehabilitation1987; 14: 321-9.13. Kuboki T, Okamoto S, Suzuki H, Kanyama M, ArakawaH, Sonoyama W, et al. Quality of life assessment of boneanchoredfixed partial denture patients with unilateralmandibular distal-extension edentulism. Journal ofProsthetic Dentistry 1999; 82: 182-7.562Indian Journal of Multidisciplinary Dentistry, Vol. 2, <strong>Issue</strong> 4, <strong>Aug</strong>ust-<strong>Oct</strong>ober 2012
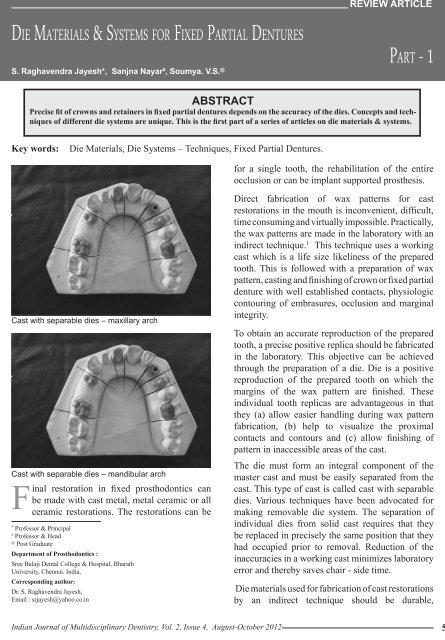
Die Materials & Sy s t e m s f o r Fixed Partial DenturesS. Raghavendra Jayesh*, Sanjna Nayar # , Soumya. V.S. @review articlePart - 1AbstractPrecise fit of crowns and retainers in fixed partial dentures depends on the accuracy of the dies. Concepts and techniquesof different die systems are unique. This is the first part of a series of articles on die materials & systems.Key words:Die Materials, Die Systems – Techniques, Fixed Partial Dentures.for a single tooth, the rehabilitation of the entireocclusion or can be implant supported prosthesis.Cast with separable dies – maxillary archCast with separable dies – mandibular archFinal restoration in fixed prosthodontics canbe made with cast metal, metal ceramic or allceramic restorations. The restorations can be*Professor & Principal#Professor & Head@Post GraduateDepartment of Prosthodontics :Sree Balaji Dental College & Hospital, BharathUniversity, Chennai. India,Corresponding author:Dr. S. Raghavendra Jayesh,Email : srjayesh@yahoo.co.inDirect fabrication of wax patterns for castrestorations in the mouth is inconvenient, difficult,time consuming and virtually impossible. Practically,the wax patterns are made in the laboratory with anindirect technique. 1 This technique uses a workingcast which is a life size likeliness of the preparedtooth. This is followed with a preparation of waxpattern, casting and finishing of crown or fixed partialdenture with well established contacts, physiologiccontouring of embrasures, occlusion and marginalintegrity.To obtain an accurate reproduction of the preparedtooth, a precise positive replica should be fabricatedin the laboratory. This objective can be achievedthrough the preparation of a die. Die is a positivereproduction of the prepared tooth on which themargins of the wax pattern are finished. Theseindividual tooth replicas are advantageous in thatthey (a) allow easier handling during wax patternfabrication, (b) help to visualize the proximalcontacts and contours and (c) allow finishing ofpattern in inaccessible areas of the cast.The die must form an integral component of themaster cast and must be easily separated from thecast. This type of cast is called cast with separabledies. Various techniques have been advocated formaking removable die system. The separation ofindividual dies from solid cast requires that theybe replaced in precisely the same position that theyhad occupied prior to removal. Reduction of theinaccuracies in a working cast minimizes laboratoryerror and thereby saves chair - side time.Die materials used for fabrication of cast restorationsby an indirect technique should be durable,Indian Journal of Multidisciplinary Dentistry, Vol. 2, <strong>Issue</strong> 4, <strong>Aug</strong>ust-<strong>Oct</strong>ober 2012 563