

Volume 2 - Issue 4 (Aug-Oct) Download Pdf - IJMD
Volume 2 - Issue 4 (Aug-Oct) Download Pdf - IJMD
Volume 2 - Issue 4 (Aug-Oct) Download Pdf - IJMD
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
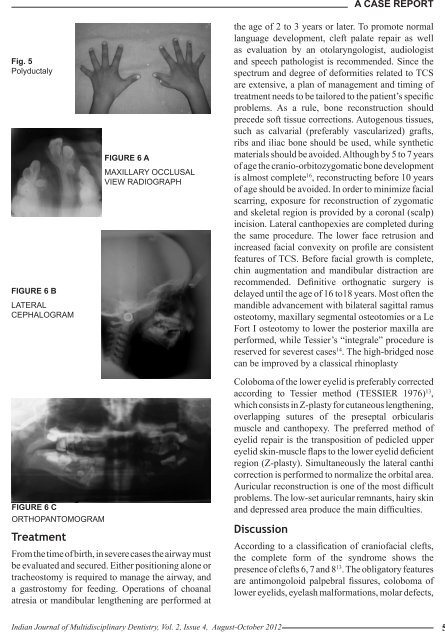
Fig. 5PolyductalyFIGURE 6 BLATERALCEPHALOGRAMFIGURE 6 AMAXILLARY OCCLUSALVIEW RADIOGRAPHA Case Reportthe age of 2 to 3 years or later. To promote normallanguage development, cleft palate repair as wellas evaluation by an otolaryngologist, audiologistand speech pathologist is recommended. Since thespectrum and degree of deformities related to TCSare extensive, a plan of management and timing oftreatment needs to be tailored to the patient’s specificproblems. As a rule, bone reconstruction shouldprecede soft tissue corrections. Autogenous tissues,such as calvarial (preferably vascularized) grafts,ribs and iliac bone should be used, while syntheticmaterials should be avoided. Although by 5 to 7 yearsof age the cranio-orbitozygomatic bone developmentis almost complete 16 , reconstructing before 10 yearsof age should be avoided. In order to minimize facialscarring, exposure for reconstruction of zygomaticand skeletal region is provided by a coronal (scalp)incision. Lateral canthopexies are completed duringthe same procedure. The lower face retrusion andincreased facial convexity on profile are consistentfeatures of TCS. Before facial growth is complete,chin augmentation and mandibular distraction arerecommended. Definitive orthognatic surgery isdelayed until the age of 16 to18 years. Most often themandible advancement with bilateral sagittal ramusosteotomy, maxillary segmental osteotomies or a LeFort I osteotomy to lower the posterior maxilla areperformed, while Tessier’s “integrale” procedure isreserved for severest cases 14 . The high-bridged nosecan be improved by a classical rhinoplastyFIGURE 6 CORTHOPANTOMOGRAMTreatmentFrom the time of birth, in severe cases the airway mustbe evaluated and secured. Either positioning alone ortracheostomy is required to manage the airway, anda gastrostomy for feeding. Operations of choanalatresia or mandibular lengthening are performed atColoboma of the lower eyelid is preferably correctedaccording to Tessier method (TESSIER 1976) 13 ,which consists in Z-plasty for cutaneous lengthening,overlapping sutures of the preseptal orbicularismuscle and canthopexy. The preferred method ofeyelid repair is the transposition of pedicled uppereyelid skin-muscle flaps to the lower eyelid deficientregion (Z-plasty). Simultaneously the lateral canthicorrection is performed to normalize the orbital area.Auricular reconstruction is one of the most difficultproblems. The low-set auricular remnants, hairy skinand depressed area produce the main difficulties.DiscussionAccording to a classification of craniofacial clefts,the complete form of the syndrome shows thepresence of clefts 6, 7 and 8 13 . The obligatory featuresare antimongoloid palpebral fissures, coloboma oflower eyelids, eyelash malformations, molar defects,Indian Journal of Multidisciplinary Dentistry, Vol. 2, <strong>Issue</strong> 4, <strong>Aug</strong>ust-<strong>Oct</strong>ober 2012 579













