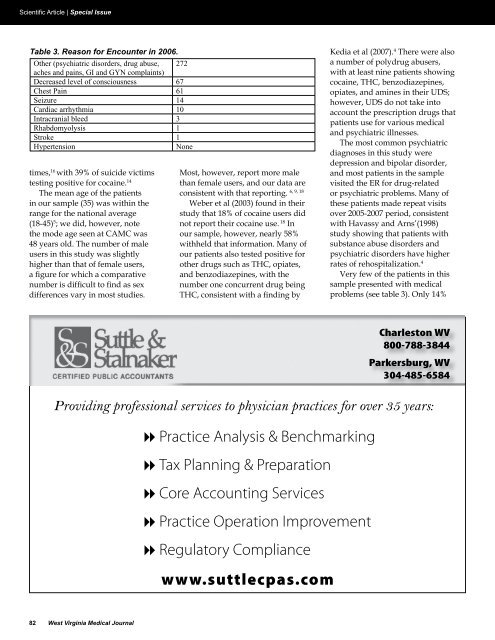
Scientific Article | Special IssueTable 3Table 3. Reason for Encounter Reason <strong>in</strong> for 2006. Encounter <strong>in</strong> 2006Other (psychiatric disorders, drug abuse, 272aches and pa<strong>in</strong>s, GI and GYN compla<strong>in</strong>ts)Decreased level of consciousness 67Chest Pa<strong>in</strong> 61Seizure 14Cardiac arrhythmia 10Intracranial bleed 3Rhabdomyolysis 1Stroke 1HypertensionNonetimes, 16 with 39% of suicide victimstest<strong>in</strong>g positive for coca<strong>in</strong>e. 14The mean age of the patients<strong>in</strong> our sample (35) was with<strong>in</strong> therange for the national average(18-45) 5 ; we did, however, notethe mode age seen at CAMC was48 years old. The number of maleusers <strong>in</strong> this study was slightlyhigher than that of female users,a figure for which a comparativenumber is difficult to f<strong>in</strong>d as sexdifferences vary <strong>in</strong> most studies.Most, however, report more malethan female users, and our data are6, 9, 18consistent with that report<strong>in</strong>g.Weber et al (2003) found <strong>in</strong> theirstudy that 18% of coca<strong>in</strong>e users didnot report their coca<strong>in</strong>e use. 18 Inour sample, however, nearly 58%withheld that <strong>in</strong>formation. Many ofour patients also tested positive forother drugs such as THC, opiates,and benzodiazep<strong>in</strong>es, with thenumber one concurrent drug be<strong>in</strong>gTHC, consistent with a f<strong>in</strong>d<strong>in</strong>g byKedia et al (2007). 4 There were alsoa number of polydrug abusers,with at least n<strong>in</strong>e patients show<strong>in</strong>gcoca<strong>in</strong>e, THC, benzodiazep<strong>in</strong>es,opiates, and am<strong>in</strong>es <strong>in</strong> their UDS;however, UDS do not take <strong>in</strong>toaccount the prescription drugs thatpatients use for various medicaland psychiatric illnesses.The most common psychiatricdiagnoses <strong>in</strong> this study weredepression and bipolar disorder,and most patients <strong>in</strong> the samplevisited the ER for drug-relatedor psychiatric problems. Many ofthese patients made repeat visitsover 2005-2007 period, consistentwith Havassy and Arns’(1998)study show<strong>in</strong>g that patients withsubstance abuse disorders andpsychiatric disorders have higherrates of rehospitalization. 4Very few of the patients <strong>in</strong> thissample presented with medicalproblems (see table 3). Only 14%Charleston <strong>WV</strong>800-788-3844Parkersburg, <strong>WV</strong>304-485-6584Provid<strong>in</strong>g professional services to physician practices for over 35 years:8 Practice Analysis & Benchmark<strong>in</strong>g8 Tax Plann<strong>in</strong>g & Preparation8 Core Account<strong>in</strong>g Services8 Practice Operation Improvement8 Regulatory Compliancewww.suttlecpas.com82 <strong>West</strong> Virg<strong>in</strong>ia <strong>Medical</strong> Journal
Special Issue | Scientific Articleof this study’s coca<strong>in</strong>e-positivepatients, <strong>in</strong> fact, presented withchest pa<strong>in</strong>, a figure far below the40% cited by McCord et al (2008). 8The retrospective nature of thisstudy constitutes a limit<strong>in</strong>g factorbecause analysis was conf<strong>in</strong>edto the <strong>in</strong>formation found <strong>in</strong> thecharts. Moreover, those data were,<strong>in</strong> part, self-reported by patients.Another limit<strong>in</strong>g factor was thatnot all patients underwent a UDS,so it is possible the study is notrepresentative of the true numberof coca<strong>in</strong>e abusers who were seen.ConclusionBased on the f<strong>in</strong>d<strong>in</strong>gs that 12% ofthe total population were trauma,further reviews would need to beperformed to determ<strong>in</strong>e if there is acorrelation between specific traumaevents and coca<strong>in</strong>e positive UDS.As noted previously, Weber etal (2003) found that 18% of theirpatients did not report drug abusewhile nearly 58% of the studypopulation did not report. Based onthese f<strong>in</strong>d<strong>in</strong>gs further <strong>in</strong>vestigationis warranted to determ<strong>in</strong>e possiblereasons beh<strong>in</strong>d the failure of thepopulation to volunteer illicitdrug abuse <strong>in</strong>formation. Possibleconclusions could be the rather“closed” Appalachian culture, fear oflaw enforcement notification, and/orignorance to the need to providesuch <strong>in</strong>formation. Additionally,the question presents if standardER protocol should <strong>in</strong>clude a UDSfor anyone who presents to the ERregardless of chief compla<strong>in</strong>t.Kedia et al (2007) reported thatpatients with substance abusedisorders and psychiatric disordershave higher rates of re-hospitalizationthan the general population 4 . Giventhe fact the majority of the population<strong>in</strong> this study presented with drugrelated and/or psychiatric issues asopposed to medically related issues,it is appropriate to conclude thereis a documented need for amplemental health resources <strong>in</strong> the ER.To the best of the researchers’knowledge this is the first studyfrom <strong>West</strong> Virg<strong>in</strong>ia which revieweda pattern of coca<strong>in</strong>e use <strong>in</strong> the ERsett<strong>in</strong>g. Despite the limitations ofthis study, the data strongly suggestthere be further <strong>in</strong>vestigation <strong>in</strong>to theutilization of UDS <strong>in</strong> the ER as wellas a review of resources availableto treat both illicit drug abuse andassociated mental health disorders.References1. Brady KT. Comorbidity With <strong>Substance</strong><strong>Abuse</strong>. Available at http://www.medscape.com/viewarticle/457178. AccessedSeptember 6, 2007.2. Dattilo PB, Hailpern SM, Fearon K, SohalD, and Nord<strong>in</strong> C. B-Blockers areAssociated with Reduced Risk ofMyocardial Infarction After Coca<strong>in</strong>e Use.Annals of Emergency Medic<strong>in</strong>e 2008;51:117-125.3. Drug Enforcement Adm<strong>in</strong>istration.Stimulants. Available from http://www.usdoj.gov/dea/pubs/abuse/5-stim.htm.Accessed July 10, 2008.4. Kedia S, Sell MA, and Relyea G. Monoversuspolydrug abuse patterns amongpublicly funded clients. <strong>Substance</strong> <strong>Abuse</strong>Treatment, Prevention, and Policy 2007.5. Kerr M. Intracranial Hemorrhage <strong>in</strong> YoungAdults L<strong>in</strong>ked to Drug <strong>Abuse</strong>. Available athttp://www.medscape.com/viewarticle/523964. Accessed September6, 2007.6. Kloner RA and Rezkalla SH. Coca<strong>in</strong>e andthe Heart. The New England Journal ofMedic<strong>in</strong>e 2003;348:487-488.7. Lange RA and Hillis LD. Cardiovascularcomplications of coca<strong>in</strong>e use. N Engl JMed. 2001;345:351-358.8. McCord J, Jneid H, Hollander JE, deLemos JA, Cercek B, Hsue P, Gibler WB,Ohman EM, Drew B, Philippides G, andNewby LK. Management of Coca<strong>in</strong>e-Associated Chest Pa<strong>in</strong> and MyocardialInfarction. A Scientific <strong>State</strong>ment From theAmerican Heart <strong>Association</strong> Acute CardiacCare Committee of the Council on Cl<strong>in</strong>icalCardiology. Circulation 2008;117.9. Moeller KE, Lee KC, and Kissack JC.Ur<strong>in</strong>e Drug Screen<strong>in</strong>g: Practical Guide forCl<strong>in</strong>icians. Mayo Cl<strong>in</strong>ic Proceed<strong>in</strong>gs2008;83:66-76.10. Office of National Drug Control Policy.Coca<strong>in</strong>e Facts and Figures. Available athttp://www.whitehousedrugpolicy.gov/drugfact/coca<strong>in</strong>e/coca<strong>in</strong>e_FF.html.Accessed July 10, 2008.11. Pavar<strong>in</strong>, RM. Coca<strong>in</strong>e consumption anddeath risk: a follow-up study on 347 coca<strong>in</strong>eaddicts <strong>in</strong> the metropolitan area of Bologna.Ann Ist Super Sanita 2008;44:91-98.12. Rezkalla SH and Kloner RA. Coca<strong>in</strong>e-Induced Acute Myocaridal Infarction.Cl<strong>in</strong>ical Medic<strong>in</strong>e & Research2007;5:172-176.13. Roy, A. Characteristics of Coca<strong>in</strong>e-Dependent Patients Who Attempt Suicide.American Journal of Psychiatry2001;158:1215-1219.14. Schuckit, MA. Drug <strong>Abuse</strong> andDependence: Epidemiology. (2006)Available at http://www.medscape.com/viewarticle/534454. Accessed September6, 2007.15. Schuckit, MA. Drug <strong>Abuse</strong> andDependence: Usual Cl<strong>in</strong>ical Course.(2006) Available at http://www.medscape.com/viewarticle/534457. AccessedSeptember 6, 200716. <strong>Substance</strong> <strong>Abuse</strong> and Mental HealthServices Adm<strong>in</strong>istration, Office of AppliedStudies. Drug <strong>Abuse</strong> Warn<strong>in</strong>g Network,2005: National Estimates of Drug-RelatedEmergency Department Visits. DAWNSeries D-29, DHHS Publication No. (SMA)07-4256, Rockville, MD, 2007.17. <strong>Substance</strong> <strong>Abuse</strong> and Mental HealthServices Adm<strong>in</strong>istration, Office of AppliedStudies. Treatment Episode Data Set(TEDS) Highlights—2006 NationalAdmissions to <strong>Substance</strong> <strong>Abuse</strong> TreatmentServices. OAS Series #S-40, DHHSPublication No. (SMA) 08-4313, Rockville,MD, 2007.18. Weber, JE, Shofer, FS, Lark<strong>in</strong>, GL, Kalaria,AS, and Hollander, JE. Validation of a BriefObservation Period for Patients withCoca<strong>in</strong>e-Associated Chest Pa<strong>in</strong>. The NewEngland Journal of Medic<strong>in</strong>e.2003;348:510-517.CME Post-Test34. Coca<strong>in</strong>e use is a serious problem? True or False35. Patients present<strong>in</strong>g to the ER with coca<strong>in</strong>e positive UDS, are seek<strong>in</strong>g medical care? True or False36. Fifty-eight percent of the ER population volunteered their illicit drug use <strong>in</strong>formation? True or FalseSUBSTANCE ABUSE IN <strong>WV</strong> | Vol. 106 83