State PATH Contacts Welcome Manual - Homelessness Resource ...
State PATH Contacts Welcome Manual - Homelessness Resource ...
State PATH Contacts Welcome Manual - Homelessness Resource ...
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
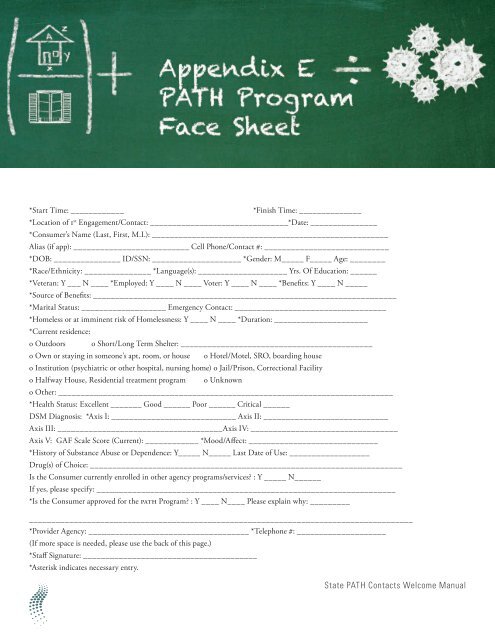
*Start Time: ____________*Finish Time: ______________*Location of 1 st Engagement/Contact: _______________________________*Date: _______________*Consumer’s Name (Last, First, M.I.): _____________________________________________________Alias (if app): __________________________ Cell Phone/Contact #: ____________________________*DOB: _______________ ID/SSN: ____________________ *Gender: M_____ F_____ Age: ________*Race/Ethnicity: _______________ *Language(s): ____________________ Yrs. Of Education: ______*Veteran: Y ___ N ____ *Employed: Y ____ N ____ Voter: Y ____ N ____ *Benefits: Y ____ N _____*Source of Benefits: ____________________________________________________________________*Marital Status: ___________________ Emergency Contact: __________________________________*Homeless or at imminent risk of <strong>Homelessness</strong>: Y ____ N ____ *Duration: _____________________*Current residence:o Outdoors o Short/Long Term Shelter: ___________________________________________o Own or staying in someone’s apt, room, or house o Hotel/Motel, SRO, boarding houseo Institution (psychiatric or other hospital, nursing home) o Jail/Prison, Correctional Facilityo Halfway House, Residential treatment program o Unknowno Other: ___________________________________________________________________________*Health Status: Excellent _______ Good ______ Poor ______ Critical ______DSM Diagnosis: *Axis I: ____________________________ Axis II: ____________________________Axis III: _____________________________________Axis IV: _________________________________Axis V: GAF Scale Score (Current): ____________ *Mood/Affect: _____________________________*History of Substance Abuse or Dependence: Y_____ N_____ Last Date of Use: __________________Drug(s) of Choice: ______________________________________________________________________Is the Consumer currently enrolled in other agency programs/services? : Y _____ N______If yes, please specify: ___________________________________________________________________*Is the Consumer approved for the <strong>PATH</strong> Program? : Y ____ N____ Please explain why: _______________________________________________________________________________________________*Provider Agency: ____________________________________ *Telephone #: ____________________(If more space is needed, please use the back of this page.)*Staff Signature: _______________________________________*Asterisk indicates necessary entry.<strong>State</strong> <strong>PATH</strong> <strong>Contacts</strong> <strong>Welcome</strong> <strong>Manual</strong>