VISION SCREENING REFERRAL - The School District of Philadelphia
VISION SCREENING REFERRAL - The School District of Philadelphia
VISION SCREENING REFERRAL - The School District of Philadelphia

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
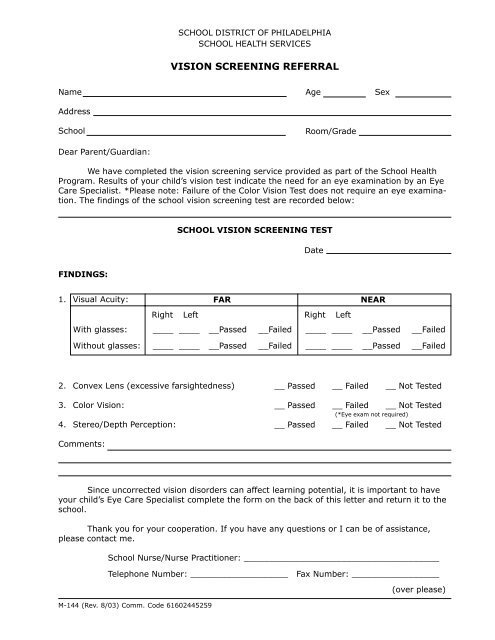
SCHOOL DISTRICT OF PHILADELPHIASCHOOL HEALTH SERVICES<strong>VISION</strong> <strong>SCREENING</strong> <strong>REFERRAL</strong>NameAddress<strong>School</strong>Dear Parent/Guardian:AgeRoom/GradeSexWe have completed the vision screening service provided as part <strong>of</strong> the <strong>School</strong> HealthProgram. Results <strong>of</strong> your child’s vision test indicate the need for an eye examination by an EyeCare Specialist. *Please note: Failure <strong>of</strong> the Color Vision Test does not require an eye examination.<strong>The</strong> findings <strong>of</strong> the school vision screening test are recorded below:SCHOOL <strong>VISION</strong> <strong>SCREENING</strong> TESTDateFINDINGS:1. Visual Acuity:FARNEARRightLeftRightLeftWith glasses:____ ______Passed__Failed____ ______Passed__FailedWithout glasses:____ ______Passed__Failed____ ______Passed__Failed2. Convex Lens (excessive farsightedness)3. Color Vision:4. Stereo/Depth Perception:__ Passed __ Failed __ Not Tested__ Passed __ Failed __ Not Tested(*Eye exam not required)__ Passed __ Failed __ Not TestedComments:Since uncorrected vision disorders can affect learning potential, it is important to haveyour child’s Eye Care Specialist complete the form on the back <strong>of</strong> this letter and return it to theschool.Thank you for your cooperation. If you have any questions or I can be <strong>of</strong> assistance,please contact me.<strong>School</strong> Nurse/Nurse Practitioner: ______________________________________Telephone Number: ___________________ Fax Number: _________________M-144 (Rev. 8/03) Comm. Code 61602445259(over please)
EYE CARE SPECIALIST REPORTStudent’s Name ____________________________________________ Date _____________Visual Acuity:FARNEARWithout correction:Right Left________Right Left________With correction:________________Diagnosis or explanation <strong>of</strong> eye condition:_________________________________________________________________________________________________________________________________________________________________________________________________________________________________________Plan <strong>of</strong> Treatment:Glasses PrescribedConstant WearNear Work OnlyDistance Work OnlyContact(s) Prescribed___ Yes___ Yes___ Yes___ Yes___ Yes___ No___ No___ No___ No___ NoRecommendation for school:Return visit:PRINT NAME OF EYE CARE SPECIALISTPLEASE RETURN THIS FORM TO SCHOOL - ATTENTION: SCHOOL NURSESIGNATURESCHOOL NAME:_____________________________________________ADDRESS: _________________________________________________TELEPHONEZIP CODE: _____________________OR FAX TO:_________________________________________________