VISION SCREENING REFERRAL - The School District of Philadelphia
VISION SCREENING REFERRAL - The School District of Philadelphia
VISION SCREENING REFERRAL - The School District of Philadelphia

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
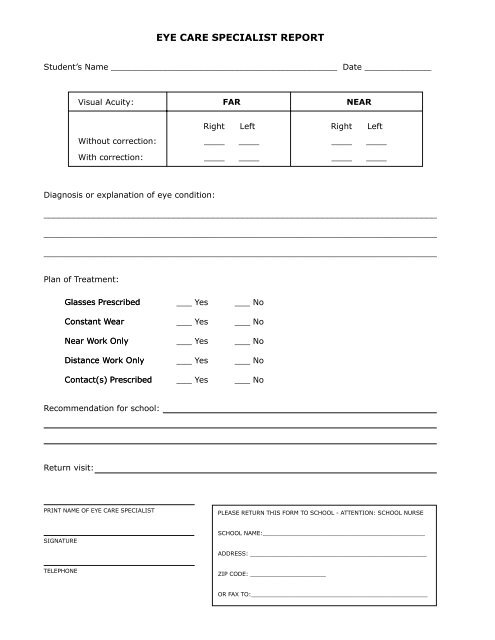
EYE CARE SPECIALIST REPORTStudent’s Name ____________________________________________ Date _____________Visual Acuity:FARNEARWithout correction:Right Left________Right Left________With correction:________________Diagnosis or explanation <strong>of</strong> eye condition:_________________________________________________________________________________________________________________________________________________________________________________________________________________________________________Plan <strong>of</strong> Treatment:Glasses PrescribedConstant WearNear Work OnlyDistance Work OnlyContact(s) Prescribed___ Yes___ Yes___ Yes___ Yes___ Yes___ No___ No___ No___ No___ NoRecommendation for school:Return visit:PRINT NAME OF EYE CARE SPECIALISTPLEASE RETURN THIS FORM TO SCHOOL - ATTENTION: SCHOOL NURSESIGNATURESCHOOL NAME:_____________________________________________ADDRESS: _________________________________________________TELEPHONEZIP CODE: _____________________OR FAX TO:_________________________________________________