VISION SCREENING REFERRAL - The School District of Philadelphia
VISION SCREENING REFERRAL - The School District of Philadelphia
VISION SCREENING REFERRAL - The School District of Philadelphia

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
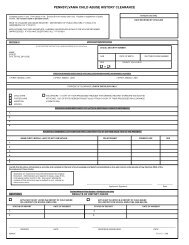
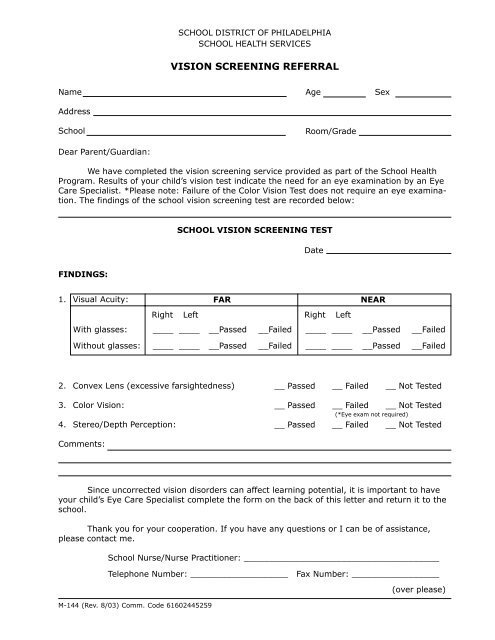
SCHOOL DISTRICT OF PHILADELPHIASCHOOL HEALTH SERVICES<strong>VISION</strong> <strong>SCREENING</strong> <strong>REFERRAL</strong>NameAddress<strong>School</strong>Dear Parent/Guardian:AgeRoom/GradeSexWe have completed the vision screening service provided as part <strong>of</strong> the <strong>School</strong> HealthProgram. Results <strong>of</strong> your child’s vision test indicate the need for an eye examination by an EyeCare Specialist. *Please note: Failure <strong>of</strong> the Color Vision Test does not require an eye examination.<strong>The</strong> findings <strong>of</strong> the school vision screening test are recorded below:SCHOOL <strong>VISION</strong> <strong>SCREENING</strong> TESTDateFINDINGS:1. Visual Acuity:FARNEARRightLeftRightLeftWith glasses:____ ______Passed__Failed____ ______Passed__FailedWithout glasses:____ ______Passed__Failed____ ______Passed__Failed2. Convex Lens (excessive farsightedness)3. Color Vision:4. Stereo/Depth Perception:__ Passed __ Failed __ Not Tested__ Passed __ Failed __ Not Tested(*Eye exam not required)__ Passed __ Failed __ Not TestedComments:Since uncorrected vision disorders can affect learning potential, it is important to haveyour child’s Eye Care Specialist complete the form on the back <strong>of</strong> this letter and return it to theschool.Thank you for your cooperation. If you have any questions or I can be <strong>of</strong> assistance,please contact me.<strong>School</strong> Nurse/Nurse Practitioner: ______________________________________Telephone Number: ___________________ Fax Number: _________________M-144 (Rev. 8/03) Comm. Code 61602445259(over please)
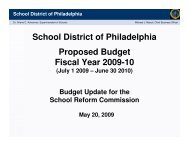
EYE CARE SPECIALIST REPORTStudent’s Name ____________________________________________ Date _____________Visual Acuity:FARNEARWithout correction:Right Left________Right Left________With correction:________________Diagnosis or explanation <strong>of</strong> eye condition:_________________________________________________________________________________________________________________________________________________________________________________________________________________________________________Plan <strong>of</strong> Treatment:Glasses PrescribedConstant WearNear Work OnlyDistance Work OnlyContact(s) Prescribed___ Yes___ Yes___ Yes___ Yes___ Yes___ No___ No___ No___ No___ NoRecommendation for school:Return visit:PRINT NAME OF EYE CARE SPECIALISTPLEASE RETURN THIS FORM TO SCHOOL - ATTENTION: SCHOOL NURSESIGNATURESCHOOL NAME:_____________________________________________ADDRESS: _________________________________________________TELEPHONEZIP CODE: _____________________OR FAX TO:_________________________________________________