Download the OSHA manual - Wisconsin Dental Association
Download the OSHA manual - Wisconsin Dental Association
Download the OSHA manual - Wisconsin Dental Association

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
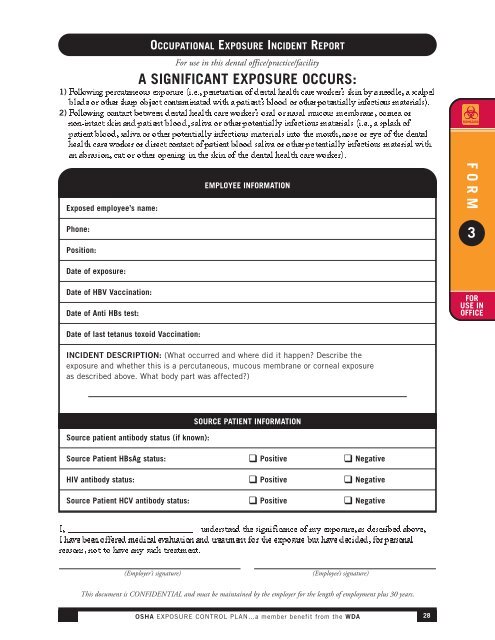
OCCUPATIONAL EXPOSURE INCIDENT REPORTFor use in this dental office/practice/facilityA SIGNIFICANT EXPOSURE OCCURS:1) Following percutaneous exposure (i.e., penetration of dental health care worker’s skin by a needle, a scalpelblade or o<strong>the</strong>r sharp object contaminated with a patient’s blood or o<strong>the</strong>r potentially infectious materials).2) Following contact between dental health care worker’s oral or nasal mucous membrane, cornea ornon-intact skin and patient blood, saliva or o<strong>the</strong>r potentially infectious materials (i.e., a splash ofpatient blood, saliva or o<strong>the</strong>r potentially infectious materials into <strong>the</strong> mouth, nose or eye of <strong>the</strong> dentalhealth care worker or direct contact of patient blood saliva or o<strong>the</strong>r potentially infectious material withan abrasion, cut or o<strong>the</strong>r opening in <strong>the</strong> skin of <strong>the</strong> dental health care worker).EMPLOYEE INFORMATIONExposed employee’s name:Phone:Position:FORM3Date of exposure:Date of HBV Vaccination:Date of Anti HBs test:FORUSE INOFFICEDate of last tetanus toxoid Vaccination:INCIDENT DESCRIPTION: (What occurred and where did it happen? Describe <strong>the</strong>exposure and whe<strong>the</strong>r this is a percutaneous, mucous membrane or corneal exposureas described above. What body part was affected?)Source patient antibody status (if known):SOURCE PATIENT INFORMATIONSource Patient HBsAg status: Positive NegativeHIV antibody status: Positive NegativeSource Patient HCV antibody status: Positive NegativeI, ____________________________ understand <strong>the</strong> significance of my exposure, as described above,I have been offered medical evaluation and treatment for <strong>the</strong> exposure but have decided, for personalreasons, not to have any such treatment.(Employer’s signature)(Employee’s signature)This document is CONFIDENTIAL and must be maintained by <strong>the</strong> employer for <strong>the</strong> length of employment plus 30 years.<strong>OSHA</strong> EXPOSURE CONTROL PLAN…a member benefit from <strong>the</strong> WDA 28