Worsening Tricuspid Regurgitation Following Pericardiectomy for ...
Worsening Tricuspid Regurgitation Following Pericardiectomy for ...
Worsening Tricuspid Regurgitation Following Pericardiectomy for ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
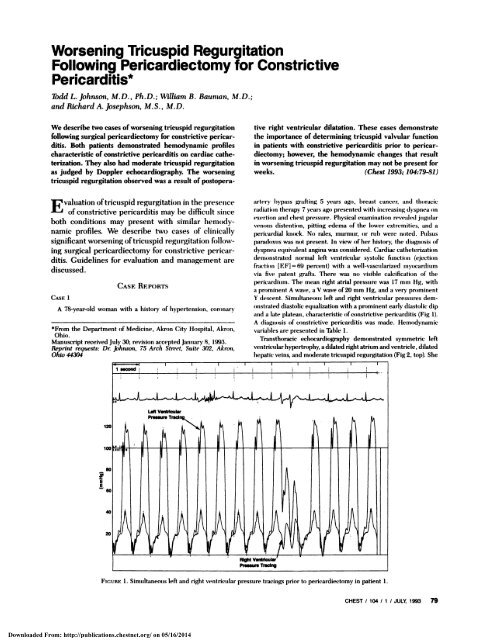
<strong>Worsening</strong> <strong>Tricuspid</strong> <strong>Regurgitation</strong><strong>Following</strong> <strong>Pericardiectomy</strong> <strong>for</strong> ConstrictivePericarditis*Todd L. Johnson, M.D. , Ph.D.; William B. Baunzan, M.D.;and Richard A. Josephson, M.S., M.D.We describe two cases of worsening tricuspid regurgitationfollowing surgical pericardiectomy <strong>for</strong> constrictive pericarditis.Both patients demonstrated hemodynamic profilescharacteristic of constrictive pericarditis on cardiac catheterization.They also had moderate tricuspid regurgitationas judged by Doppler echocardiography. The worseningtricuspid regurgitation observed was a result of postopera-E valuation oftricuspid regurgitation in the presenceof constrictive pencarditis may be difficult sinceboth conditions may present with similar hemodynamicprofiles. We describe two cases of clinicallysignificant worsening oftricuspid regurgitation followingsurgical pericardiectomy <strong>for</strong> constrictive pericarditis.Guidelines <strong>for</strong> evaluation and management arediscussed.CASE 1CASEREPORTSA 78-year-old woman with a history of hypertension, coronary*Fmm the Department of Medicine, Akron City Hospital, Akron,Ohio.Manuscript received July 30; revision accepted January 8, 1993.Reprint rrquests: Dr. Johnson, 75 Arch Street, Suite 302, Akron,Ohio 44304five right ventricular dilatation. These cases demonstratethe importance of determining tricuspid valvular functionin patients with constrictive pericarditis prior to pericardiectomy;however, the hemodynamic changes that resultin worsening tricuspid regurgitation may not be present <strong>for</strong>weeks. (Chest 1993; 104:79-81)artery bypass grafting 5 years ago, breast cancer, and thoracicradiation therapy 7 years ago presented with increasing (hyspnea onexertion and chest pressure. Physical examination revealed jugularvenous distention, pitting edema of the lower extremities, and apericardial knock. No rales, murmur, or rub were noted. Pulsusparadoxus was not present. In view of her history, the diagnosis ofdyspnea equivalent angina was considered. Cardiac catheterizationdemonstrated normal left ventricular systolic function (ejectionfraction [EF] = 69 percent) with a well-vasculanized myocardiumvia five patent grafts. There was no visible calcification of thepenic’ardmm. The mean right atnal pressure was 17 mm Hg, witha prominent A wave, a V wave of2O mm Hg, and a very prominentY descent. Simultaneous left and right ventricular pressures demonstrateddiastolic equalization with a prominent early diastolic dipand a late plateau, characteristic of constrictive penicarditis (Fig 1).A diagnosis of constrictive pericarditis was made. Hemodynamicvariables are presented in Table 1.Transthoracic echocardiography demonstrated symmetric leftventricular hypertrophy, adilated right atrium and ventricle, dilatedhepatic veins, and moderate tricuspid regurgitation (Fig 2, top). SheEEFIGURE 1 . Simultaneous left and right ventricular pressure tracings prior to pericardiectomy in patient 1.CHEST I 104 I 1 I JULY, 1993 79Downloaded From: http://publications.chestnet.org/ on 05/16/2014
Table 1-Hemodynamw Variables Prior to <strong>Pericardiectomy</strong>*LV Pressure, mm Hg RV Pressure, mm Hg PAP, mm Hg CO. L/min CI, Llmin/m2Patient 1 123/20 40/20 31118 3.9 1.9Patient2 129/18 55/18 52/17 4.9 2.6*LV = left ventricle; RV right ventricle; PAP pulmonary artery pressure; CO cardiac output; CI cardiac index.was discharged from the hospital on a regimen of the following: L-thyroxine, 0.05 mg orally every day; furosemide, 40 mg orally everyday; enalapnil, 2.5 mg orally every day; diltiazem SR, 90 mg orallyevery day; and aspirin, 325 mg orally every day. Despite medicaltreatment, the patient returned with dyspnea and lower extremityedema. Physical examination revealed jugular venous distension,ascites, and pitting edema of the lower extremities. No rales,murmur, rub, or knock were detected. The patient subsequentlyunderwent visceral pericardiectomy 4 weeks after the initialpresentation. A left anterolateral thoracotomy incision was utilizedin view of her previous coronary artery bypass grafting. Thepericardium was noted to appear thin intraoperatively.During the procedure, the right ventricle was noted to expandand the cardiac output improved from 3.3 to 4.0 L/min. Excisionwas believed to be complete, with dissection from phrenic nerve::#{149}:L:: i’..: -t14#{149}1$FIGURE 2. Top: Jet of tricuspid regurgitation prior to pericardiectomy,patient 1 . Bottom: Jet of tricuspid regurgitation followingpericardiectomy, patient 1.to phrenic nerve. Pathologic evaluation ofthe penicardium revealedfibromembranous tissue with fibrosis and mild nonspecific chronicinflammation. Immediately postoperatively, the patient’s right atrialpressure tracing was noted to undergo ventricularization. Thepatient was discharged from the hospital 10 days later on a regimenof the following: L-thyroxine, 0.10 mg orally every day; diltiazem,60 mg orally every day; enalapril, 2.5 mg orally every day;furosemide, 40 mg orally every day; and aspirin, 325 mg orallyevery day. The patient was readmitted to the hospital 4 weeks laterwith increasing dyspnea and fatigue. Physical examination revealedmassive edema of the lower extremities and lower back, moderatejugular venous distention, bibasilar rales, and no gallop but a grade2/6 systolic murmur heard best at the upper left sternal border. Achest radiograph revealed slight cardiomegaly and some accentuationof the perihilar and upper lobe vascularity. A transthoracicechocardiogram revealed severe tricuspid regurgitation, with reversalofflow in the hepatic veins (Fig2, bottom). <strong>Tricuspid</strong> annuloplastywas subsequently per<strong>for</strong>med. An intraoperative transesophagealechocardiogram demonstrated severe tricuspid regurgitation dueto a dilated tricuspid annulus. The right ventricle demonstratednormal wall motion. All of the tricuspid leaflets were intact with noruptured or elongated chordae noted intraoperatively. Annuloplastywith a No. 34 Carpentier ring was successful. In follow-up, thepatient felt well and was walking up stairs without difficulty. Onexamination there was no peripheral edema, the neck veins wereflat, and the lungs were clear to auscultation.CASE 2An 83-year-old man with a history of prostatic cancer presentedto the emergency department with a complaint of shortness ofbreath. Physical examination was remarkable <strong>for</strong> moderate jugularvenous distention, no rales, no gallop, and pitting edema to theknees bilaterally. A chest radiograph revealed bilateral free-movingpleural effusions, moderate cardiomegaly, metastatic lesions in theribs, and equalization of pulmonary vascular flow suggestive ofslight pulmonary venous hypertension. An electrocardiogram revealeda normal sinus rhythm with a rate of 75, and low voltage inthe frontal plane leads. Transthoracic echocardiogram demonstrateda dilated right atrium and ventricle, normal systolic function, andmoderate tricuspid regurgitation (Fig 3, top). Cardiac cathetenizationdemonstrated normal left ventricular function and no visiblepericardial calcification. The mean right atrial pressure was 17 mmHg with a prominent A and V wave, as well as a steep X and Ydescent. Simultaneous left and right ventricular pressures demonstrateddiastolic equalization with a dip and plateau pattern.Hemodynamic variables are presented in Table 1 . The patientsubsequently underwent visceral pericardiectomy via a mediansternotomy incision. Excision was thought to be complete fromphrenic nerve to phrenic nerve. The heart appeared normal andthe pencardium was noted to appear slightly thickened. Pathologicevaluation of the pericardium revealed fibrosis with focal areas ofslight chronic inflammation.The patient was extubated on postoperative day 3 and underwentdiuresis <strong>for</strong> pulmonary edema. A 30-mm C-V wave was noted onright atrial tracing and the patient developed a murmur consistentwith tricuspid regurgitation. Two days later the patient’s appetitedecreased, he had occasional bouts of nausea and vomiting, hismental status deteriorated, and he developed ascites. A transesophagealechocardiogram was per<strong>for</strong>med which demonstrated80 <strong>Worsening</strong> <strong>Tricuspid</strong> <strong>Regurgitation</strong> (Johnson, Bauman, Josephson)Downloaded From: http://publications.chestnet.org/ on 05/16/2014
- , t:..-“. :: -_cE,9: ; - a: z.. _.4,.a. z_- : .A_’__ I’ :- .- i . 4 _\ I \ \ . \ 4,_-The hemodynamics ofboth patients were characteristicof constrictive pericarditis, demonstrating rapidearly diastolic ventricular filling, equalization of leftand right ventricular diastolic pressures and normalventricular systolic function. Both patients also hadmoderate tricuspid regurgitation be<strong>for</strong>e pericardiectomyas judged by Doppler echocardiography. Hemodynamicstudies months after pericardiectomytypically demonstrate decreased right atrial, rightventricular, pulmonary artery and pulmonary capillarywedge 1,2 Decreases in central venouspressure tend to occur after 2 to 4 days postoperativelyand reach normal by 4 weeks.2 The etiology of thepersistence ofabnormal end-diastolic ventricular pres-‘-#{149}1sures in the early postoperative period is unclear. Ithas been suggested that the abnormal ventricularcompliance is due to myocardial alterations. Anatomicstudies in cases of constrictive pericarditis have demonstratedmyocardial atrophy.4 During pericardiectomy,the right ventricle frequently visibly expands.5The worsening tricuspid regurgitation observed inthese patients following pericardiectomy demonstratesthat in some cases, the right ventricle maydilate to the point that severe tricuspid regurgitationoccurs.These cases demonstrate the importance of determiningtricuspid valvular function in patients withconstrictive pencarditis prior to pericardiectomy. Iftricuspid regurgitation is present preoperatively, acombined procedure, ie, tricuspid annuloplasty andpericardiectomy, may be needed . Intraoperativetransesophageal echocardiography may aid in thisdecision; however, as in case 1 , the hemodynamicchanges that result in worsened tricuspid regurgitationmay not be present until much later.FIGURE 3. Top: Jet of tricuspid regurgitation prior to pericardiectomy,patient 2. Bottom: Jet of tricuspid regurgitation followingpenicardiectomy, patient 2.normal left and right ventricular wall motion, right ventriculardilatation, and severe tricuspid regurgitation (Fig 3, bottom) with acalculated pulmonary artery systolic pressure of 71 mm Hg. Thepatient was believed to be a poor surgical candidate <strong>for</strong> annuloplastyand in fact refused surgery. He died 3 days later. An autopsy wasnotper<strong>for</strong>med.DISCuSsIoNREFERENCES1 Kloster FE, Cnslip RL, Bnistow JD, Herr RH, Ritzmann LW,Griswold HE. Hemodynamic studies following pericardiectomy<strong>for</strong> constrictive pericarditis. Circulation 1965; 32:415-242 Viola AR. The influence ofpericardiectomy on the hemodynamicsofchronic constrictive pericarditis. Circulation 1973; 48:1038-423 Deterling BA, Humphreys GH. Factors in the etiology ofconstrictive penicarditis. Circulation 1955; 12:30-434 Dines DE, Edwards JE, Burchell WB. Myocardial atrophy inconstrictive penicarditis. Mayo Clin Proc 1958; 33:93-95 Bashi \TM John 5, Ravikumar E, Jairaj PS, Shyamsunder K,Krishnaswami S. Early and late results ofpericardiectomy in 118cases ofconstnictive pericarditis. Thorax 1988; 43:637-41CHEST I 104 I 1 I JULY, 1993 81Downloaded From: http://publications.chestnet.org/ on 05/16/2014