

Delivering the 18 Weeks Referral to Treatment Standard Output Report
Delivering the 18 Weeks Referral to Treatment Standard Output Report
Delivering the 18 Weeks Referral to Treatment Standard Output Report

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Dental Specialties Task and Finish Group<strong>Delivering</strong> <strong>the</strong> <strong>18</strong> <strong>Weeks</strong> <strong>Referral</strong> <strong>to</strong> <strong>Treatment</strong> <strong>Standard</strong> forDental Specialties<strong>Output</strong> <strong>Report</strong>January 2011
ContentsIntroduction 4Foreword 4Chair’s Reflections 6Context 7<strong>18</strong> <strong>Weeks</strong> <strong>Referral</strong> <strong>to</strong> <strong>Treatment</strong> <strong>Standard</strong> 7The <strong>18</strong> <strong>Weeks</strong> National Delivery Structure 7Task and Finish Groups 7Dental Specialties Task and Finish Group 8Dental Specialties’ Supply and Demand 9Current Waiting Times 10Identified Risks <strong>to</strong> Delivery 11Priority Task and Finish Group Improvement Actions 11Planning and Delivery 13Profile 13Measurement Considerations 13Monthly Management Information 14<strong>Treatment</strong>s in Outpatient Departments 15Clinical Outcome <strong>Report</strong>ing 15Frequently Asked Questions and Scenarios 16Applying <strong>the</strong> Definitions 17Action Planning – Undergraduate <strong>Treatment</strong>s <strong>18</strong>Demand, Capacity, Activity, Queue Analysis <strong>18</strong>Health Intelligence 19Influencing <strong>Referral</strong> Processes 24Dental Specialties Task & Finish Group – January 2011 2
Demand is not a given 24Effective <strong>Referral</strong> Management 25Advice Only <strong>Referral</strong>s 26Early <strong>Referral</strong>s 27Pathway Approach: Philosophy 27<strong>Referral</strong> Management Pathways for Orthodontics and Oral Surgery 28Index of Orthodontic <strong>Treatment</strong> Need 28Res<strong>to</strong>rative Dentistry 29Scottish Dental Needs Assessment Programme 29Managing Patient Flows 30Servie Redesign and Transformation 31Tele-dentistry 32Dental Specialties’ Workforce Skills Mix 34Workforce Solutions Workshop 35Communication 37Stakeholder Groups 37National Events 37Conclusion: Action Planning and Ongoing Work 38Summary of Fundamental Next Steps for Boards 39Appendix One: Membership of Dental Specialties Task and Finish Group 41Appendix Two: Key Areas for Improvement 41Appendix Three: Orthodontic <strong>Referral</strong> Management Pathway Group 43Appendix Four: Oral Surgery <strong>Referral</strong> Management Pathway Group 44Appendix Five: Orthodontic Pathway and <strong>Referral</strong> Guidance 44Appendix Six: Oral Surgery Pathway and <strong>Referral</strong> Guidance 47Appendix Seven: Who is doing what Matrix 49Dental Specialties Task & Finish Group – January 2011 3
IntroductionForewordThe work of <strong>the</strong> Dental Specialties Task and Finish Group has been sponsored by<strong>the</strong> Scottish Government’s <strong>18</strong> <strong>Weeks</strong> <strong>Referral</strong> <strong>to</strong> <strong>Treatment</strong> (RTT) OperationalDelivery Team, and ultimately by <strong>the</strong> Scottish Government’s Health DeliveryDirec<strong>to</strong>rate. The Task and Finish Group, has, from a national perspective,considered how identified risks <strong>to</strong> delivery across <strong>the</strong>se specialties may beproactively managed, and this report details outputs of this work.The core elements listed below are commended <strong>to</strong> you by <strong>the</strong> Operational DeliveryTeam for action. Every Board is <strong>the</strong>refore expected <strong>to</strong> ensure that each aspect isfully explored, progressed and embedded appropriately across <strong>the</strong>ir HealthCommunity <strong>to</strong> support timely and high quality patient care. It is essential that allopportunities for streamlined service management and ongoing improvement andtransformation are optimised, with <strong>the</strong> patient’s interest right at <strong>the</strong> centre. Deliveryand improvement require whole systems ownership and strong organisationalleadership – both clinical and managerial – in order <strong>to</strong> operationalise change on asustainable basis. For dental specialties, much of this will take place at <strong>the</strong>primary/secondary care interface, as well as requiring a continuing focus on differentways of working in <strong>the</strong> acute secondary care sec<strong>to</strong>r.The core elements commended <strong>to</strong> Health Communities and NHS Boards forearly action are:1. Ensure high organisational profile of, and clear delivery expectations inrelation <strong>to</strong> Dental Specialties, with integration in<strong>to</strong> Boards’ existing deliverysystems for all o<strong>the</strong>r specialties, including waiting times performancemoni<strong>to</strong>ring and management, service redesign and pathway work.2. Proactively pursue accurate and fit for purpose data capture and its uselocally as a key source of health intelligence. Information should be used forservice planning, including managing <strong>the</strong> balance of capacity and demand; forhighlighting actions needed for service improvement; and for performancemanagement of waiting times targets. Accurate measurement of <strong>18</strong> weeksRTT for Dental Specialties is also reliant on <strong>the</strong> uniform application of ‘clockstarts’ and ‘clock s<strong>to</strong>ps’ which are set out in detail in <strong>the</strong> Dental Definitions &Scenarios : http://www.<strong>18</strong>weeks.scot.nhs.uk/how-<strong>to</strong>-achieve-and-maintain-<strong>18</strong>-weeks/task-and-finish-groups/dental-specialties/3. Drive uniform implementation of <strong>the</strong> agreed common pathways forOrthodontics and Oral Surgery, and ensure <strong>the</strong>se are embedded right across<strong>the</strong> health community on a sustainable basis, <strong>to</strong> support equity of access andcare. Implementation of <strong>the</strong>se pathways as commended, will also influencereferral practices and referral thresholds, and engagement should <strong>the</strong>reforebe initiated with stakeholders across <strong>the</strong> whole care system <strong>to</strong> promoteadherence <strong>to</strong> <strong>the</strong> pathways.Dental Specialties Task & Finish Group – January 2011 4
4. Make <strong>the</strong> most of your workforce, by evaluating <strong>the</strong> responsibilities andcompetencies of <strong>the</strong> multidisciplinary team, and proactively enhancing <strong>the</strong>skills-mix of o<strong>the</strong>r professionals <strong>to</strong> complement existing roles and functions.It is expected that health communities will continue <strong>to</strong> develop and improvesecondary care dental services and pathways locally; <strong>the</strong>re is still much <strong>to</strong> do <strong>to</strong>safeguard sustainable and timely service provision. The Improvement and SupportTeam will continue <strong>to</strong> provide support <strong>to</strong> Boards in achieving <strong>the</strong> <strong>18</strong> <strong>Weeks</strong> <strong>Referral</strong><strong>to</strong> <strong>Treatment</strong> target. The Summary of Fundamental Next Steps for Boards on page39 may provide useful guidance for service redesign.Should performance across any of <strong>the</strong> dental specialties prove unsatisfac<strong>to</strong>ry, <strong>the</strong>escalation process triggered by <strong>the</strong> Scottish Government could include fur<strong>the</strong>r actionplanning with <strong>the</strong> Access Support Team, more detailed tailored support, interventionas needed and submission of detailed recovery plans.Robert CalderwoodChair of <strong>the</strong> <strong>18</strong> <strong>Weeks</strong> Operational Delivery TeamDental Specialties Task & Finish Group – January 2011 5
Chair’s ReflectionsHis<strong>to</strong>rically <strong>the</strong>re has perhaps been a feeling that Dental Specialties are lessimportant, or are considered <strong>to</strong> be a specialty sidelined from <strong>the</strong> main stream. Thisis not true. The quality and timeliness of patient care and <strong>the</strong> patient experienceremain paramount in all specialties, and <strong>the</strong> waiting times standards apply.Dental Specialties are not different.The <strong>18</strong> <strong>Weeks</strong> RTT <strong>the</strong>refore provides an opportunity, as well as a challenge, <strong>to</strong>bring secondary care dental specialties on<strong>to</strong> a par with all o<strong>the</strong>r organisationallearning and established systems and processes already embedded in o<strong>the</strong>rspecialties, <strong>to</strong> ensure that all dental specialties are fully empowered <strong>to</strong> provide highquality and timely patient care on an ongoing basis.The best way <strong>to</strong> start addressing <strong>the</strong> issues is <strong>to</strong> begin with <strong>the</strong> basics and work up<strong>to</strong> ensure all <strong>the</strong> foundations are firmly laid which in some cases can bring somequick wins.In its discussions <strong>the</strong> Task and Finish Group considered some of <strong>the</strong> elements thatare generic across all dental specialties. O<strong>the</strong>r elements and issues consideredpertain <strong>to</strong> specific dental specialties. This approach is reflected in this report <strong>to</strong>o.Derek LeslieChair of <strong>the</strong> Dental Specialties Task and Finish GroupDental Specialties Task & Finish Group – January 2011 6
Context<strong>18</strong> <strong>Weeks</strong> <strong>Referral</strong> <strong>to</strong> <strong>Treatment</strong> <strong>Standard</strong>The Cabinet Secretary for Health and Wellbeing has pledged “a whole journeywaiting time of <strong>18</strong> <strong>Weeks</strong> from…referral <strong>to</strong> treatment by December 2011.”This applies equally <strong>to</strong> all specialties provided in secondary care, and <strong>the</strong>reforeincludes Dental Specialties.<strong>18</strong> <strong>Weeks</strong> will <strong>the</strong>refore be <strong>the</strong> maximum wait from receipt of referral in<strong>to</strong> secondarycare, <strong>to</strong> <strong>the</strong> start of <strong>the</strong> first definitive treatment, for all non-emergency conditions.The <strong>18</strong> <strong>Weeks</strong> National Delivery StructureIn order <strong>to</strong> ensure a cohesive approach between <strong>the</strong> Scottish Government andHealth Boards in <strong>the</strong> delivery of this target, while ensuring high quality patientfocussed care is maintained, a national delivery approach was established. The <strong>18</strong><strong>Weeks</strong>’ Programme Board oversees <strong>the</strong> work of four Delivery Teams – focussing onInformation, Emergency Access, Operational Issues, and Diagnostics. The detailedinvolvement of key stakeholders and ‘change-champions’ in this process brings aninformed mix of knowledge, expertise and experience <strong>to</strong> each specialist area.Task and Finish GroupsAs a consequence of analyses undertaken through <strong>the</strong> Operational Delivery Team, anumber of Task and Finish Groups were set up <strong>to</strong> concentrate on those specialtiesregarded as most at risk <strong>to</strong> delivering <strong>the</strong> <strong>18</strong> <strong>Weeks</strong> <strong>Referral</strong> <strong>to</strong> <strong>Treatment</strong> Target.Each of <strong>the</strong>se short life working groups consists of a small number of expert advisors- clinicians, service managers and additional professionals involved in that specialty;<strong>the</strong> groups are also supported by members from <strong>the</strong> Scottish Government’s HealthDelivery Direc<strong>to</strong>rate. The first five ‘at risk’ specialties <strong>to</strong> see <strong>the</strong> establishment of aTask and Finish Group were: Audiology, Dental Specialties, Neurological Services,Orthopaedics and Plastic Surgery. More recently Task and Finish Groups have alsobeen established for Derma<strong>to</strong>logy, Diagnostics and Capacity / DemandManagement. Although each of <strong>the</strong> Task and Finish Groups focus on particularissues relating <strong>to</strong> that specialty area, all groups work from a series of common workstrands, namely:• Measurement and Definitions• Demand/Capacity/Activity/Queue Analysis• Demand Side Solutions• Performance Management• Service Redesign and Transformation• Culture/Change• Workforce• CommunicationDental Specialties Task & Finish Group – January 2011 7
Dental Specialties Task and Finish GroupThe Dental Specialties Task and Finish Group had its first meeting in September2008, and ran as a short-life working group until September 2010. Membership islisted as Appendix One.The Task and Finish Group recognises <strong>the</strong> differences in service delivery between<strong>the</strong> different dental specialties; however, this output report picks out common <strong>the</strong>mesand approaches which largely apply, as well as specifics for <strong>the</strong> different specialties.Mythbusting:Fact: All Dental Specialties must deliver <strong>the</strong> <strong>18</strong> <strong>Weeks</strong> <strong>Referral</strong> <strong>to</strong> <strong>Treatment</strong> targetby 31 December 2011. There are no exceptions.Dental Specialties included within <strong>the</strong> <strong>18</strong> <strong>Weeks</strong> RTT <strong>Standard</strong> are:• Orthodontics;• Res<strong>to</strong>rative Dentistry;• Oral Surgery;• Oral Medicine;• Paediatric Dentistry; and• All Dental Procedures carried out under General Anaes<strong>the</strong>tic.Maxillofacial Surgery (in or out of <strong>18</strong> <strong>Weeks</strong> RTT?)Maxillofacial surgery is technically not classified as a Dental Specialty and <strong>the</strong>reforeis outwith <strong>the</strong> remit of <strong>the</strong> Dental Specialties Task and Finish Group. Much of <strong>the</strong>activity within this discipline is linked <strong>to</strong> Oral Surgery and <strong>the</strong>refore it is difficult <strong>to</strong>extricate <strong>the</strong> two. Clinicians and o<strong>the</strong>r stakeholders have <strong>the</strong>refore adopted anintegrated approach. Regardless, <strong>the</strong> <strong>18</strong> Week <strong>Referral</strong> <strong>to</strong> <strong>Treatment</strong> target stillapplies.Community and Salaried Dental Services (in or out of <strong>18</strong> <strong>Weeks</strong> RTT?)The complexities of patterns of service delivery in <strong>the</strong> different care settings are wellrecognised, influenced by <strong>the</strong> financial and o<strong>the</strong>r drivers which come in<strong>to</strong> play. Theconsequent interaction between <strong>the</strong> different parts of <strong>the</strong> service can have asignificant impact on <strong>the</strong> provision of care.Never<strong>the</strong>less, consultations and treatment carried out by general dentalpractitioners, community dental practitioners or by specialist practitioners workingwithin <strong>the</strong> community and salaried services are not part of <strong>the</strong> <strong>18</strong> <strong>Weeks</strong> <strong>Referral</strong> <strong>to</strong><strong>Treatment</strong> target.There are, however, two exceptions when community based interventions arepart of <strong>the</strong> <strong>18</strong> <strong>Weeks</strong> RTT <strong>Standard</strong>:Dental Specialties Task & Finish Group – January 2011 8
1. The planned procedure which is being carried out in <strong>the</strong> community is undertakenby a secondary care specialist.2. The procedure requires a General Anaes<strong>the</strong>tic.In <strong>the</strong>se circumstances <strong>the</strong> intervention will be included in <strong>the</strong> <strong>18</strong> <strong>Weeks</strong> RTT target.Fur<strong>the</strong>r clarification is given in <strong>the</strong> Dental Specialties Frequently Asked Questions:http://www.<strong>18</strong>weeks.scot.nhs.uk/how-<strong>to</strong>-achieve-and-maintain-<strong>18</strong>-weeks/task-andfinish-groups/dental-specialties/Dental Specialties’ Supply and DemandThe Task and Finish Group firmly recognises <strong>the</strong> variation in service supply indifferent parts of <strong>the</strong> country and acknowledges <strong>the</strong> affect that this can have uponmodels of care within different health communities and ultimately, where treatmentsare provided.It is recognised that some parts of <strong>the</strong> country do not have <strong>the</strong> same level ofpractitioners across primary and community care as o<strong>the</strong>rs. In particular <strong>the</strong>re isevidence of variation between central belt and <strong>the</strong> North of Scotland, such asperhaps more limited independent sec<strong>to</strong>r provision in <strong>the</strong> North.Similarly some parts of <strong>the</strong> country, often remote and rural areas, find it difficult <strong>to</strong>attract General Dental Practitioners. Within General Dental Practice itself, serviceprovision varies, for example a high street general dental practitioner may treat ei<strong>the</strong>rNHS or private patients, or both. This creates varying dynamics and patient flowsacross different health communities.As a consequence, in some geographic areas, <strong>the</strong>re is more reliance upon <strong>the</strong>primary care salaried dental services (PCSDS) <strong>to</strong> provide fundamental dentaltreatment.As a result of such variation, alternative approaches <strong>to</strong> care have been adopted. Forexample, Forth Valley has two specialist orthodontic practices, which has had asignificant impact on keeping secondary care lists shorter, whilst Dumfries andGalloway has established an alternative model of care based around <strong>the</strong>ir primarycare centres. In <strong>the</strong> North of Scotland, a Primary Care Specialist in Oral Surgerytakes referrals directly from General Practice, which creates ano<strong>the</strong>r different modelof care.Thus, a range of fac<strong>to</strong>rs impact on <strong>the</strong> supply of care within <strong>the</strong> primary andcommunity setting, and can result in a high level of demand for basic dental care <strong>to</strong>be provided within acute secondary care. This creates an imbalance of supply anddemand, which can result in long waiting times for some dental specialties.Patient flows are fur<strong>the</strong>r affected in that currently just under 70% of Scotland’s adultpopulation is registered with a General Dental Practitioner. The remaining 30% are<strong>the</strong>refore perhaps more likely <strong>to</strong> present <strong>to</strong> secondary care regardless of <strong>the</strong> severityof <strong>the</strong>ir condition.Dental Specialties Task & Finish Group – January 2011 9
during a return outpatient appointment. This is <strong>to</strong> be encouraged, but in manyinstances, current reporting systems mean that <strong>the</strong>se treatments are not recorded aspart of <strong>the</strong> activity. Similarly currently <strong>the</strong>y do not always ‘s<strong>to</strong>p a clock’ as part ofmeasuring patient waiting times.One of <strong>the</strong> key challenges <strong>to</strong> <strong>the</strong>se specialties <strong>the</strong>refore, is capturing and measuring,and <strong>the</strong>n delivering all elements of <strong>the</strong> patient journey. This should facilitate anunderstanding and management of <strong>the</strong> true stage of treatment waiting times in order<strong>to</strong> make progressive improvements <strong>to</strong> reducing waiting times.By reducing <strong>the</strong> component parts of <strong>the</strong> patient journey (i.e. outpatients, inpatients,daycases), achievement of <strong>the</strong> whole pathway, from receipt of referral <strong>to</strong> <strong>the</strong> start ofdefinitive treatment, within <strong>18</strong> weeks becomes more manageable. It is this deliveryrequirement that <strong>the</strong> Task and Finish Group has focused upon, across all <strong>the</strong>specialties, and continue <strong>to</strong> address <strong>the</strong> identified risks <strong>to</strong> delivery and <strong>the</strong>consequent challenges and opportunities as a core part of its outputs.Identified Risks <strong>to</strong> DeliveryFrom its inception, <strong>the</strong> Task and Finish Group highlighted a range of challenges forearly consideration:1. Long waiting times in some dental specialties.2. Interface between primary and secondary care and <strong>the</strong> financial drivers that canaffect this.3. Variations in referral practices and differing treatment pathways across <strong>the</strong> caresettings for a single condition (e.g. simple extraction of <strong>to</strong>oth).4. Variations in referral thresholds, especially for orthodontic treatments.5. Establishment of robust data collection and reporting systems <strong>to</strong> proactivelymanage dental specialties and associated waiting times.6. Uniform application of <strong>the</strong> definitions <strong>to</strong> ensure consistent and accurate recordingof patient journey times.7. Hidden waits for treatments undertaken in <strong>the</strong> outpatient setting which were notpreviously measured.8. Workforce considerations and fur<strong>the</strong>r use of enhanced practitioner roles.9. Organisational profile and integration of dental specialties in<strong>to</strong> waiting timesmanagement processes.Priority Task and Finish Group Improvement ActionsAs part of <strong>the</strong> methodology for minimising <strong>the</strong>se risks, <strong>the</strong> Dental Specialties Taskand Finish Group identified <strong>the</strong> following priority actions for <strong>the</strong> Group:Dental Specialties Task & Finish Group – January 2011 11
1. Ensuring high organisational profile of, and clear delivery expectations in relation<strong>to</strong> Dental Specialties, with integration in<strong>to</strong> Boards’ existing delivery systems for allo<strong>the</strong>r specialties.2. A critical success fac<strong>to</strong>r in <strong>the</strong> delivery of <strong>18</strong> weeks RTT is clearly recognisingthat <strong>18</strong> weeks applies equally <strong>to</strong> all Dental Specialties as <strong>to</strong> any o<strong>the</strong>r specialty.3. Embedding learning from o<strong>the</strong>r specialties regarding delivery e.g. <strong>the</strong>fundamental principles of waiting list management.4. Proactively pursuing accurate and fit for purpose data capture and its use locallyas a key source of health intelligence.5. Setting out and <strong>the</strong>n encouraging <strong>the</strong> uniform application of ‘clock starts’ and‘clock s<strong>to</strong>ps’ <strong>to</strong> facilitate <strong>the</strong> accurate measurement of <strong>18</strong> <strong>Weeks</strong> RTT for dentalspecialties.6. Ensuring accurate recording of treatments undertaken in an outpatient setting(including return outpatient appointments) so clocks are s<strong>to</strong>pped once firstdefinitive treatment is commended.7. Developing common pathways for Orthodontics and Oral Surgery, and drivinguniform implementation <strong>to</strong> ensure <strong>the</strong>se are embedded right across <strong>the</strong> healthcommunity on a sustainable basis.8. Highlighting workforce opportunities in order <strong>to</strong> proactively enhance <strong>the</strong> skills-mixof o<strong>the</strong>r professionals <strong>to</strong> complement existing roles and functions.Dental Specialties Task & Finish Group – January 2011 12
Planning and DeliveryProfileThe organisational profile of Dental Specialties and <strong>the</strong> associated expectations ofdelivery are critical <strong>to</strong> <strong>the</strong> achievement of <strong>the</strong> waiting times targets and <strong>the</strong> provisionof high quality patient care.The Task and Finish Group has worked <strong>to</strong> raise <strong>the</strong> profile of Dental Specialties insecondary care and <strong>to</strong> emphasise <strong>the</strong>ir inclusion in <strong>the</strong> <strong>18</strong> <strong>Weeks</strong> <strong>Referral</strong> <strong>to</strong><strong>Treatment</strong> <strong>Standard</strong>.Boards are asked <strong>to</strong> ensure that dental specialties are fully integrated in<strong>to</strong> all aspectsof <strong>the</strong>ir <strong>18</strong> weeks RTT work, especially generic workstreams on information,performance moni<strong>to</strong>ring and management, service redesign and pathway work.This will facilitate organisational learning and <strong>the</strong> adoption and spread of goodpractice waiting times management and delivery (i.e. reduce a tendency <strong>to</strong> reinvent<strong>the</strong> wheel).Dental Specialties should also be a standard part of each organisations’ regulardelivery management meetings, underpinned by high level leadership and support <strong>to</strong>address bottlenecks and improve access <strong>to</strong> services.MythbustingFact: Dental Specialties are no different <strong>to</strong> o<strong>the</strong>r acute specialties and are expected<strong>to</strong> deliver <strong>to</strong> <strong>the</strong> national waiting times standards.Action Planning - Waiting Times Delivery ProcessesNHS Boards should continue <strong>to</strong> mainstream Dental Specialties in<strong>to</strong> establishedwaiting times delivery processes, and learn from good practice approaches.Measurement ConsiderationsOne of <strong>the</strong> initial actions of <strong>the</strong> Task and Finish Group was <strong>to</strong> assess waiting timesinformation provided <strong>to</strong> <strong>the</strong> Information Services Division (ISD). The Task and FinishGroup has identified significant concerns with <strong>the</strong> existing data available for dentalspecialties. Although Boards have his<strong>to</strong>rically provided some Stage of <strong>Treatment</strong>data in <strong>the</strong>ir submissions <strong>to</strong> ISD, this is not deemed complete or sufficiently robust <strong>to</strong>fully inform day-<strong>to</strong>-day management and improvement actions. Validation systemsand processes are not embedded, and <strong>the</strong> data must <strong>the</strong>refore be treated withcaution.Dental Specialties Task & Finish Group – January 2011 13
In order <strong>to</strong> progress <strong>the</strong>se issues outlined above, ISD convened an internal ‘dentalinformation group’. This group has initially focussed on <strong>the</strong> fur<strong>the</strong>r analysis of currentdata <strong>to</strong> ascertain its completeness and accuracy.As part of this approach, <strong>the</strong> Task and Finish Group continue <strong>to</strong> prioritiseengagement with colleagues from ISD <strong>to</strong> support all stakeholders in developingmethodologies for accurately capturing data. Work continues <strong>to</strong> identify andestablish improved measurement and data collection systems for all dentalspecialties, based on locally-derived information sources. Such a data set isessential <strong>to</strong> provide a sustainable measurement and reporting system that can beused for three primary purposes – for service planning, for service improvement andfor performance management, each at <strong>the</strong> local, regional and national levels.Discussions at <strong>the</strong> data masterclass held on 28 th September 2009 provided a fur<strong>the</strong>rinsight in<strong>to</strong> how existing data sources and collection systems might be improved andaugmented. As well as performance management, o<strong>the</strong>r fac<strong>to</strong>rs that will help focus<strong>the</strong> need for comprehensive data were identified as:• Managing Did Not Attend (DNA) rates.• Assessing variation in referral rates by general dental practices.• Understanding who could potentially be best treated in primary care or insecondary care.• Ensuring general anaes<strong>the</strong>tics are recorded for all patients, irrespective of whomretains responsibility for <strong>the</strong> patient.Action Planning - Data CollectionHealth Boards need <strong>to</strong> action and embed a robust and sustainable measurementand reporting system that can be used at different levels for service planning, forimproving <strong>the</strong> patient journey and for performance management. NHS Boards need<strong>to</strong> consider how <strong>the</strong>y mainstream this information for everyday operational use.Monthly Management InformationAs an interim approach, pending measurement of <strong>the</strong> full <strong>18</strong> <strong>Weeks</strong> journey, NHSBoards have been asked <strong>to</strong> use <strong>the</strong>ir local intelligence <strong>to</strong> provide Dental MonthlyManagement Information (MMI). Specifically, Health Boards have been asked <strong>to</strong>complete information on <strong>the</strong> number of new patients waiting longer than 9 and 12weeks for assessment in <strong>the</strong> outpatient setting and <strong>the</strong> number of patients waitinglonger than 9 and <strong>18</strong> weeks for return out-patient treatments, covering <strong>the</strong> fiveDental Specialties and General Anaes<strong>the</strong>tics. At present though, not all HealthBoards are regularly submitting <strong>the</strong>ir spreadsheet, and not all those received arecomplete. Fur<strong>the</strong>r emphasis on completion and accuracy of this information hasbecome critical; without this it is difficult <strong>to</strong> significantly progress performance,service redesign and improvement. To support this process, and <strong>to</strong> build on existingorganisational learning <strong>the</strong> Dental Monthly Management Information should becompiled, verified and submitted centrally by each Board’s information departmentalong with <strong>the</strong> main MMI.Dental Specialties Task & Finish Group – January 2011 14
Action Planning - Dental MMINHS Boards should create drivers <strong>to</strong> ensure <strong>the</strong> collection and submission of <strong>the</strong>Dental Monthly Management Information (MMI), co-ordinated by <strong>the</strong>ir InformationDepartment.<strong>Treatment</strong>s in Outpatient DepartmentsA cause for increasing concern is <strong>the</strong> high proportion of dental treatmentsundertaken within an outpatient setting that are not recorded. Often, only <strong>the</strong>outpatient first assessment and inpatient or daycase treatment is recorded but not<strong>the</strong> treatment activity specifically undertaken as a return outpatient, nor <strong>the</strong> length ofwait and time of ‘clock s<strong>to</strong>p’ for this cohort of patients. The waiting times targets stillapply <strong>to</strong> this group of patients, but due <strong>to</strong> such measurement difficulties it has notalways been possible <strong>to</strong> tightly manage <strong>the</strong>m. Long waits are been reportedanecdotally and urgent data capture is needed <strong>to</strong> understand <strong>the</strong> activity required <strong>to</strong>treat this group of patients within national waiting times.Action Planning - Data CaptureThere is an urgent need <strong>to</strong> ensure accurate data capture of all treatmentsundertaken within an outpatient setting, <strong>to</strong> ensure compliance with national waitingtimes.Clinical Outcome <strong>Report</strong>ingThe uniform application of clinical outcome reporting is an important aspect ofcapturing Dental treatment undertaken in an outpatient setting. Even if this iscaptured initially on paper, <strong>the</strong> resulting intelligence should be electronicallyrecorded, manipulated and interrogated. Work continues via <strong>the</strong> Improvement andSupport Team (IST) and local <strong>18</strong> <strong>Weeks</strong> RTT teams <strong>to</strong> ensure that clinical outcomesare recorded within Health Boards, across all specialties.A number of Boards are already diligently completing <strong>the</strong>ir clinical outcomes across<strong>the</strong> Dental Specialties; o<strong>the</strong>rs need <strong>to</strong> roll out this system more widely. Local auditsof completeness and accuracy of <strong>the</strong> data captured a) on paper, and b)electronically, are being considered in some areas.Action Planning - Clinical OutcomesEnsure capture of your clinical outcome codes for all stages of <strong>the</strong> patient journey -first assessment and return outpatient appointments whe<strong>the</strong>r for treatment or review.As part of <strong>the</strong> <strong>18</strong> <strong>Weeks</strong> RTT <strong>Standard</strong>, <strong>to</strong> be achieved by December 2011, wholejourney measurement must be developed for Dental Specialties in line with all o<strong>the</strong>rDental Specialties Task & Finish Group – January 2011 15
services. The national targets for both non-admitted and admitted datacompleteness and performance and ongoing improvement in, and reliance on, <strong>the</strong>sewhole journey measures continues <strong>to</strong> receive a high priority nationally.MythbustingFact: Dental Specialties are part of <strong>18</strong> <strong>Weeks</strong> RTT reporting and must <strong>the</strong>refore bepart of <strong>the</strong> whole journey data completeness process in Boards.Members of <strong>the</strong> Dental Specialties Task and Finish Group continue <strong>to</strong> work withcolleagues from ISD <strong>to</strong> help NHS Boards create a robust data capture system for allparts of <strong>the</strong> journey, and particularly in <strong>the</strong> measurement of waiting times for returnout-patient treatments.Given this essential requirement for robust and fit-for-purpose data and information,a ‘Dental Specialties Data Quality Improvement Group’ has recently beenestablished, based on a model previously used for New Ways and Audiology dataquality improvement. This group will focus on working proactively with keystakeholders in NHS Boards <strong>to</strong> improve and embed Dental Specialties informationand understanding. Initially this revolves around a scoping exercise <strong>to</strong> ascertainnational and local data requirements and <strong>the</strong>n <strong>to</strong> identify systems and processes forcollecting and verifying data capture for detailed use at a number of levels.Action Planning - Local Information ExpertiseUse local expertise within your Board’s information department <strong>to</strong> helpsupport and improve Dental Specialties data quality, data collection and analysis.Frequently Asked Questions and ScenariosThe application of common definitions is fundamental <strong>to</strong> <strong>the</strong> accurate measuremen<strong>to</strong>f waiting times in all specialties, including dentistry. The generic clock start/s<strong>to</strong>pdefinitions apply, as set out in <strong>18</strong> <strong>Weeks</strong>: The <strong>Referral</strong> <strong>to</strong> <strong>Treatment</strong> <strong>Standard</strong> –Principles and Definitions (issue 2.0, January 2009).http://www.<strong>18</strong>weeks.scot.nhs.uk/how-<strong>to</strong>-measure-and-moni<strong>to</strong>rperformance/principles-and-definitions/The Information Delivery Team advises that this document is currently being revised.The Task and Finish Group has compiled a series of Frequently Asked Questions(FAQs), with a view <strong>to</strong> enhancing <strong>the</strong> understanding of how <strong>the</strong> <strong>18</strong> <strong>Weeks</strong> RTTPrinciples and Definitions apply <strong>to</strong> Dental Specialties. The challenge is <strong>to</strong> apply <strong>the</strong>principles and definitions universally.The Dental Definitions & Scenarios is intended <strong>to</strong> address any inconsistencies inunderstanding and common application of <strong>the</strong> definitions right across NHSScotland,Dental Specialties Task & Finish Group – January 2011 16
and may be accessed at: : http://www.<strong>18</strong>weeks.scot.nhs.uk/how-<strong>to</strong>-achieve-andmaintain-<strong>18</strong>-weeks/task-and-finish-groups/dental-specialties/MythbustingFact: <strong>18</strong> <strong>Weeks</strong> RTT applies <strong>to</strong> <strong>the</strong> five secondary care Dental Specialties andGeneral Anaes<strong>the</strong>tics, namely:• Paediatric Dentistry• Orthodontics• Res<strong>to</strong>rative• Oral Surgery• Oral Medicine• General Anaes<strong>the</strong>ticsApplying <strong>the</strong> DefinitionsAn <strong>18</strong> weeks journey is measured from receipt of referral in<strong>to</strong> secondary care, <strong>to</strong> <strong>the</strong>start of definitive treatment. It is important that all localities continue <strong>to</strong> apply andrecord <strong>the</strong> clock starts, pauses and s<strong>to</strong>ps in <strong>the</strong> same way. The measurement clockstarts on date of receipt of referral in<strong>to</strong> secondary care. The clock s<strong>to</strong>ps at <strong>the</strong> star<strong>to</strong>f first definitive treatment.An ongoing programme of treatment, once commenced, is not part of <strong>18</strong> weeks RTTmeasurement. However it is a fundamental aspect of service provision and important<strong>to</strong> recognise in capacity planning.Additionally, <strong>the</strong>re are occasions when a clock will be paused or reset. These aredescribed in <strong>the</strong> Dental Definitions and Scenarios.MythbustingFact: An <strong>18</strong> Week journey is measured from receipt of referral in<strong>to</strong> secondary care,<strong>to</strong> <strong>the</strong> start of definitive treatment. Accurate and uniform application of clock startsand s<strong>to</strong>ps will ensure that journeys do not seem longer than <strong>the</strong>y actually are.Patients who choose <strong>to</strong> be reviewed and treated in a Dental School as part of anundergraduate training programme are not subject <strong>to</strong> <strong>the</strong> <strong>18</strong> <strong>Weeks</strong> RTT standard.This is because assessments and treatments required for training purposes may notnecessarily be required <strong>to</strong> be treated in a secondary care setting. Additionally,patients may experience a longer wait <strong>to</strong> accommodate <strong>the</strong> timing of <strong>the</strong>undergraduate curriculum.However, if a patient is seen in <strong>the</strong> Dental School by any o<strong>the</strong>r grade <strong>the</strong>ir waitingtime clock will continue <strong>to</strong> count down until <strong>the</strong>ir first definitive treatment is delivered.Dental Specialties Task & Finish Group – January 2011 17
MythbustingFact: Procedures performed by undergraduate dental students are not covered by<strong>the</strong> <strong>18</strong> <strong>Weeks</strong> RTT <strong>Standard</strong>.Action Planning – Undergraduate <strong>Treatment</strong>sSystems should be set in place <strong>to</strong> ensure that patients are aware of <strong>the</strong>ir exclusionfrom <strong>18</strong> <strong>Weeks</strong> RTT when opting <strong>to</strong> be treated as part of <strong>the</strong> Undergraduate TrainingProgramme.Demand, Capacity, Activity, Queue AnalysisAccurate data input and capture of <strong>the</strong> resulting health intelligence is integral <strong>to</strong>robust demand, capacity, activity, queue (DCAQ) analysis. Understanding, and <strong>the</strong>nmanaging, <strong>the</strong> balance of capacity and demand for each of <strong>the</strong> secondary careDental Specialties is fundamental <strong>to</strong> every health system’s ability <strong>to</strong> deliver.Action Planning - Managing Capacity and DemandUndertake Demand, Capacity, Activity and Queue (DCAQ) analysis for each DentalSpecialty in order <strong>to</strong> understand and <strong>the</strong>n manage <strong>the</strong> balance of capacity anddemand.Boards need <strong>to</strong> prioritise DCAQ management for <strong>the</strong>ir Dental Specialties, ensuringthat all actions are taken which may influence this. Important elements <strong>to</strong> considerand carefully manage include <strong>the</strong> proactive management of seasonal variations,booking systems and treating routine patients in turn.In order <strong>to</strong> deliver a sustainable and equitable service across secondary care DentalSpecialties, it may be necessary <strong>to</strong> undertake some one-off backlog removal <strong>to</strong> bringservices in<strong>to</strong> balance. However, this should only be done on <strong>the</strong> basis of achieving asustainable balance between capacity and demand, ensuring that continuousoptimal use is made of <strong>the</strong> resources available. The Task and Finish Group hasidentified a range of areas where <strong>the</strong> uniform application of good practice will offeractivity gains and as a result of working smarter, not harder, an increased level ofactivity may be achieved.Action Planning- Board Capacity PlansDevelop a detailed local capacity plan including managing variation, making betteruse of available capacity, and where appropriate one off back-logremoval.Dental Specialties Task & Finish Group – January 2011 <strong>18</strong>
NHS Boards can utilise <strong>the</strong> following <strong>to</strong>ols <strong>to</strong> help manage DCAQ:• Waiting List and booking Process Demonstra<strong>to</strong>r:http://www.nodelaysscotland.scot.nhs.uk/Resources/ResourceGuideItems/Pages/ISTWaitingListBookingProcessDemonstra<strong>to</strong>r.aspx• Capacity and Queue Calcula<strong>to</strong>rhttp://www.nodelaysscotland.scot.nhs.uk/Resources/ResourceGuideItems/Pages/CapacityandQueueCalcula<strong>to</strong>r.aspxHealth IntelligenceThe following charts provide an assessment of <strong>the</strong> risk as of June 2010 <strong>to</strong> showsome of <strong>the</strong> variations in supply and demand <strong>to</strong> be overcome. These are sourcedfrom Information Services Division’s QueSsTCap information, which analyses queueshape, size, trend and capacity using national waiting times data. This informationoffers an important insight in<strong>to</strong> <strong>the</strong> balance of capacity and demand for secondarycare Dental Services, and an indication of how sustainable <strong>the</strong> current lengths ofwait are likely <strong>to</strong> be.Dental Specialties Task & Finish Group – January 2011 19
Figure 1: New Outpatients on <strong>the</strong> Waiting List1. Total number of patients on <strong>the</strong> waiting list at month end (census)New Outpatients - NHS Scotland - Oral Medicine1400120010008006004002000Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov DecSource:New Ways data, as at 30 Jun 20102008 2009 2010Using Oral Medicine as an example, this graph shows <strong>the</strong> <strong>to</strong>tal number of patientson <strong>the</strong> waiting list for a first appointment during 2008, 2009, and up <strong>to</strong> and includingJune 2010. This shows that <strong>the</strong>re was a greater number of patients on waiting listsin 2008, whereas 2009 and 2010 gives reduced numbers.Since March 2010, all source referrals form part of <strong>the</strong> <strong>18</strong> <strong>Weeks</strong> <strong>Referral</strong> <strong>to</strong><strong>Treatment</strong> <strong>Standard</strong>. These include referrals received from an individual, team,service or organisation on behalf of a patient, or a patient may refer him/herself.Typical referral sources <strong>to</strong> secondary care include:• Accident and Emergency Department• Emergency Dental Service• General Dental Practitioner• General Medical Practitioner• Salaried Primary Care Dental PractitionerDental Specialties Task & Finish Group – January 2011 20
Figure 2: Distribution of Waits3502. Distribution of ongoing waits at Jun 2010New Outpatients - NHS Scotland - OrthodonticsAll <strong>Referral</strong> Sources30025043%33%200<strong>18</strong>%1506%1005000
Figure 3: Additions and Removals3003. Waiting List Activity - Additions <strong>to</strong> list & removals from list within monthInpatients - NHS Scotland - Oral Surgery250200150100500-50-100-150Jan 2008Feb 2008Mar 2008Apr 2008May 2008Jun 2008Jul 2008Aug 2008Sep 2008Source:New Ways data, as at 30 Jun 2010Oct 2008Nov 2008Dec 2008Jan 2009Feb 2009Mar 2009Apr 2009May 2009Jun 2009Jul 2009Aug 2009Sep 2009Oct 2009Nov 2009Dec 2009Jan 2010Feb 2010Mar 2010Apr 2010May 2010Jun 2010Gap betw een additions/removals Additions <strong>to</strong> list Removals <strong>to</strong> listThis graph illustrates variation in additions and removals from <strong>the</strong> waiting list in <strong>the</strong>specialty of Oral Surgery. It highlights some months where removals did not balanceadditions and waiting lists grew, or vice versa. Overall it highlights a relative balancebetween capacity and demand. It is essential for NHS Boards <strong>to</strong> understand <strong>the</strong>irown variation and plan sustainable capacity accordingly.Dental Specialties Task & Finish Group – January 2011 22
Figure 4: <strong>Weeks</strong> <strong>to</strong> Clear4.b) Estimated <strong>to</strong>tal number of weeks <strong>to</strong> clear Waiting List at month endbased on monthly activityNew Outpatients - NHS Scotland - Orthodontics by month14.012.48.99.99.59.79.68.38.57.29.89.87.612.010.08.06.04.02.00.0Jul2009Aug2009Sep2009Oct2009Nov2009Dec2009Jan2010Feb2010Mar2010Apr2010May2010Jun2010<strong>Weeks</strong> <strong>to</strong> clear allow ing for unavailabilityPeriods of unavailabilitySource:Total w eeks <strong>to</strong> clear = w eeks <strong>to</strong> clear allow ing for unavailability + average w eeksNew Ways data, as at 30 Jun 2010Using orthodontics as an example, this graph calculates <strong>the</strong> indicative number ofweeks required <strong>to</strong> clear <strong>the</strong> new outpatient waiting list for NHSScotland based on<strong>the</strong>ir recent activity. This is a measure of all activity including waiting list initiativesas well as core activity. If <strong>the</strong> indicative number of weeks required <strong>to</strong> clear <strong>the</strong> list issignificantly greater than <strong>the</strong> stage of treatment target (e.g. 12 weeks) this indicatesrisk; if <strong>the</strong> indicative number of weeks <strong>to</strong> clear is less than <strong>the</strong> stage of treatmenttarget this does not guarantee <strong>the</strong>re is no risk – for example, activity could be beingincreased by unsustainable waiting list initiatives.It is important for boards <strong>to</strong> understand <strong>the</strong> level of activity required for ‘business asusual’, i.e. <strong>to</strong> meet appropriate demand as opposed <strong>to</strong> <strong>the</strong> one-off activity requiredfor ‘back-log clearance.’Toge<strong>the</strong>r this health intelligence must be used at a local level <strong>to</strong> understand <strong>the</strong>detail of specialty queues, size and shape, <strong>the</strong> balance of additions and removalsfrom <strong>the</strong> list, and weeks <strong>to</strong> clear. Each element, and <strong>the</strong> combined effect areessential building blocks of capacity / demand management which must beproactively used for each dental specialty <strong>to</strong> maximise capacity gains and keep <strong>the</strong>service in balance.Dental Specialties Task & Finish Group – January 2011 23
Influencing <strong>Referral</strong> ProcessesPart of <strong>the</strong> philosophy of NHSScotland is ensuring that each patient is seen by <strong>the</strong>right professional, in <strong>the</strong> right care setting, at <strong>the</strong> right time, first time. This maxim isparticularly relevant <strong>to</strong> dental specialties where a variety of patient pathways for <strong>the</strong>same condition have been witnessed. This may be addressed <strong>to</strong> a great extent byadopting standardised pathways as described in <strong>the</strong> section ‘Pathway Approach -Philosophy’, but also by influencing <strong>the</strong> referral process in<strong>to</strong> secondary care, with <strong>the</strong>patient right at <strong>the</strong> heart of this. It is <strong>the</strong>refore important <strong>to</strong> understand who iscoming in<strong>to</strong> secondary care, why are <strong>the</strong>y coming in, is this <strong>the</strong> best place for <strong>the</strong>patient <strong>to</strong> be, and what are <strong>the</strong> influencing fac<strong>to</strong>rs for each referral?Demand is not a givenIt has been suggested that a high proportion of patients are assessed and treated in<strong>the</strong> wrong care setting.In 2007-2008 approximately 45% of oral surgery procedures performed in one NHSBoard were coded as ‘simple’ extraction of <strong>to</strong>oth. Simple extractions can beperformed in <strong>the</strong> primary/community care setting which would reduce demand onhospital services.Simple extractions are often referred <strong>to</strong> oral surgery departments within secondarycare, as some General Dental Practitioners (GDPs) refer in, choosing not <strong>to</strong>undertake this procedure <strong>the</strong>mselves. Variation in service supply in different parts of<strong>the</strong> country and <strong>the</strong> impact that this may have upon models of care within differen<strong>the</strong>alth communities has already been recognised. However, <strong>the</strong>re remains scope fordeveloping a clearer understanding of referral patterns by practice, along withvariation in rates of referral for different dental conditions. The outputs of this workcould be used locally <strong>to</strong>:• Develop referral thresholds, which should usefully be linked <strong>to</strong> clinical standardsabout where thresholds lie.• Influence <strong>the</strong> type and <strong>the</strong> quality of referrals e.g. tick box stationery.• Explore <strong>the</strong> scope for increased continuing professional development, educationand training <strong>to</strong> overcome recurrent referrals in specific areas.• Feedback <strong>to</strong> origina<strong>to</strong>rs regarding <strong>the</strong> quality of referrals and data regarding <strong>the</strong>purpose and timeliness of referrals.• Discuss different referral patterns with outlying practices <strong>to</strong> consider alternativeapproaches.This is occurring in o<strong>the</strong>r clinical specialties and is <strong>the</strong> subject of one of <strong>the</strong>workstreams of <strong>the</strong> Capacity / Demand Management Task and Finish Group. It hasDental Specialties Task & Finish Group – January 2011 24
also been recognised that <strong>the</strong>re may be regional approaches that could be initiated<strong>to</strong> overcome variation in <strong>the</strong> nature of referrals <strong>to</strong> secondary care.MythbustingFact: Demand in<strong>to</strong> secondary care is not a given: it can be driven down. Anysecondary care practitioner has <strong>the</strong> right <strong>to</strong> refer a patient back <strong>to</strong> <strong>the</strong> referrer e.g. if<strong>the</strong> procedure would be more appropriately carried out within <strong>the</strong> primary orcommunity care setting, or if alternative care pathways can be initiated.Effective <strong>Referral</strong> ManagementThere is likely <strong>to</strong> be fur<strong>the</strong>r scope for shifting <strong>the</strong> balance of care by proactivelytriaging patients and reinforcing appropriateness of patient flows. An example ofgood practice in <strong>the</strong> area of referral management and triage is Greater Glasgow andClyde’s <strong>Referral</strong> Hub within <strong>the</strong>ir Dental Hospital.Sharing Good Practice - Glasgow Dental Hospital (GDH)In 2007, an electronic referral pilot was commenced for referring patients from <strong>the</strong>General Dental Service (GDS) <strong>to</strong> acute Dental Services. The aspiration is that allreferrals <strong>to</strong> acute salaried and community dental services are made <strong>to</strong> a virtualreferral centre for triage <strong>to</strong> <strong>the</strong> most appropriate location. The key benefit of this isthat referrers know <strong>the</strong> referral has been received. The recipients are provided withcomprehensive information that allows efficient triage. Manda<strong>to</strong>ry fields must becompleted, <strong>the</strong>reby ensuring relevant demographic and clinical information isincluded.To date all specialties can now be referred <strong>to</strong> acute services using <strong>the</strong> electronicreferral. 50 GDS and Salaried and Community Dental Service (SCDS) locations canuse electronic referrals with a fur<strong>the</strong>r 50 poised <strong>to</strong> go live in early 2011. In addition,daily vetting has now been established for paper and electronic referrals whichensures prompt appointing <strong>to</strong> <strong>the</strong> appropriate clinic.Training is scheduled for clinicians and health records staff for electronic triage. Thiswill have additional benefits for GDS, as <strong>the</strong> referrer will be able <strong>to</strong> view on screenwhen <strong>the</strong> patient has been triaged and appointed <strong>to</strong> a clinic.Currently GDH are also pursuing <strong>the</strong> possibility of ensuring that SCDS locations canhave <strong>the</strong>ir clinics included on <strong>the</strong> acute hospital’s patient information system. Thiswill allow patients for acute services and SCDS <strong>to</strong> be referred <strong>to</strong> GDH. The referralswould <strong>the</strong>n be triaged electronically <strong>to</strong> <strong>the</strong> most appropriate locations.Pro<strong>to</strong>cols will be developed <strong>to</strong> ensure consistency in triage. This currently is in placefor referrals <strong>to</strong> adult sedation services where all patients are referred <strong>to</strong> GlasgowDental Hospital and <strong>the</strong>n triaged by a Consultant and a Salaried GDP before beingappointed (for assessment and treatment) <strong>to</strong> <strong>the</strong> most appropriate clinic. Fullinformation will be provided <strong>to</strong> referrers on which groups of patients each SCDSclinic treats. Clinic templates will be reviewed and systems for cancellation andDental Specialties Task & Finish Group – January 2011 25
changes <strong>to</strong> templates will be made, consistent with <strong>the</strong> acute services, in terms ofcomplete introduction of 6 weeks clinic cancellation policy across all services.There are some challenges associated with this service. The roll out of <strong>the</strong> electronicpilot has been slow, partly as a consequence of <strong>the</strong> unavailability of CHI <strong>to</strong> <strong>the</strong>referrers. This has resulted in health records staff having <strong>to</strong> input this informationmanually on receipt of referrals. Dental reference files are not routinely updated in<strong>the</strong> same way that GMP files are, <strong>the</strong>refore this also impacts on health records staff.These issues are being addressed.More recent issues raised (as a result of asking GDPs with access <strong>to</strong> electronicreferrals why <strong>the</strong>y do not consistently use <strong>the</strong>m), are IT issues. Whilst practices werefunded for N3 connection with one PC per practice, <strong>the</strong> PC tends <strong>to</strong> be at receptionand additional PCs in surgeries are not always connected <strong>to</strong> <strong>the</strong> same network.The project has been supported by IM&T staff who have been <strong>the</strong> key links withGDS staff.Advice Only <strong>Referral</strong>sIt should be acknowledged that secondary care practitioners are under no obligation<strong>to</strong> see and assess all patients referred. To see all comers for assessment can createa ‘revolving-door syndrome’, confuse patient expectations, undermine <strong>the</strong> quality of<strong>the</strong> patient experience and can swamp available capacity with a knock on effect ono<strong>the</strong>r users of <strong>the</strong> service.In o<strong>the</strong>r specialties, a clinician may refer a patient directly back <strong>to</strong> General Practicewith advice for fur<strong>the</strong>r care in a community setting, if <strong>the</strong> patient is not ready fortreatment or if <strong>the</strong> referral threshold applied is not appropriate for secondary care.In some instances, referrals in<strong>to</strong> secondary care can be made in order <strong>to</strong> obtain acare plan, which may <strong>the</strong>n be carried out in primary care. Therefore, <strong>the</strong>re may bescope for fur<strong>the</strong>r development of an ‘advice-only’ route, which does not necessitate<strong>the</strong> patient presenting for assessment in secondary care and ‘using up’ a clinic slotand does not start <strong>the</strong> <strong>18</strong> <strong>Weeks</strong> RTT ‘clock.’This practice offers an important feedback loop for professionals and facilitates eachpatient receiving <strong>the</strong>ir care in <strong>the</strong> most appropriate care setting. This has becomestandard practice and can be supported by referral pro<strong>to</strong>cols for specific conditions.A number of NHS Boards set this out clearly in <strong>the</strong>ir Service Information Direc<strong>to</strong>ry,and engage in ongoing dialogue with individual practices should <strong>the</strong>y showsignificant variation in <strong>the</strong>ir approach <strong>to</strong> referrals.Action Planning – Advice OnlyConsider developing an ‘advice-only’ route, which does not necessitate <strong>the</strong> patientpresenting for assessment in secondary care and ‘using up’ a clinic slot and does notstart <strong>the</strong> <strong>18</strong> <strong>Weeks</strong> RTT ‘clock.’Dental Specialties Task & Finish Group – January 2011 26
Early <strong>Referral</strong>sA referral should only be made when a patient is symp<strong>to</strong>matically ready fortreatment. Existing referral practice as a result of his<strong>to</strong>rically lengthy waits forassessment and treatment across Dental Specialties has however resulted inreferrers making early referrals in<strong>to</strong> secondary care in an attempt <strong>to</strong> counteract <strong>the</strong>likelihood of a long wait. Additionally some referrers make referrals when <strong>the</strong> patientis not orally fit <strong>to</strong> undergo a procedure or commence treatment.Consequently, artificially high numbers of patients are listed at any one time. Thissituation can be exacerbated by dual referrals <strong>to</strong> two different services in an effort <strong>to</strong>combat anticipated long waits. This used <strong>to</strong> be <strong>the</strong> case in many o<strong>the</strong>rs specialties,but with a steady reduction in waiting times, <strong>the</strong>re has been a linked reduction in <strong>the</strong>perceived need for referrers <strong>to</strong> refer early. Patients should only be referred <strong>to</strong>secondary care once <strong>the</strong>y are ready for treatment. A patient referred prematurelyshould be referred back <strong>to</strong> <strong>the</strong>ir GDP or GP for referral at <strong>the</strong> appropriate point intime.MythbustingFact: Patients should not be on waiting lists unless <strong>the</strong>y are fit <strong>to</strong> commencetreatment.Action Planning – Early <strong>Referral</strong>sEnsure that any patient referred prematurely or inappropriately is referred back <strong>to</strong><strong>the</strong>ir GDP or GP <strong>to</strong> be re-referred at a more appropriate time.Pathway Approach: PhilosophyThe Task and Finish Group, along with o<strong>the</strong>r stakeholders, have highlightedsignificant variation between patient pathways for individuals with <strong>the</strong> samecondition. Whilst <strong>the</strong>re may be clinical reasons for variation, in <strong>the</strong> main it isconsidered that variation is normally <strong>the</strong> result of o<strong>the</strong>r drivers, such as individualGDPs referral practices, <strong>the</strong> length of individual consultant’s waiting list or financialinfluences for ei<strong>the</strong>r <strong>the</strong> practitioner or <strong>the</strong> patient. It is also acknowledged that manypatients assessed and treated in secondary care dentistry, may be moreappropriately cared for in <strong>the</strong> community setting.Equity of access for all patients should be a fundamental consideration, and <strong>the</strong>reremains fur<strong>the</strong>r scope for changes in <strong>the</strong> way which patient journeys are managedand <strong>the</strong> care setting in which this occurs. This may be managed through a pathwayapproach using a common schematic <strong>to</strong> standardise or streamline <strong>the</strong> patientjourney whenever appropriate, minimising bottlenecks and smoothing handoffs.Dental Specialties Task & Finish Group – January 2011 27
<strong>Referral</strong> Management Pathways for Orthodontics and Oral SurgeryThe Task and Finish Group commissioned two focused referral managementpathway groups for Orthodontics and Oral Surgery, <strong>to</strong> develop and agree astreamlined pathway approach. As well as reducing unnecessary variation intreatment plans for <strong>the</strong> same condition, <strong>the</strong> pathways aim <strong>to</strong> facilitate more equitablereferral patterns and common thresholds for referrals <strong>to</strong> secondary care.Each pathway group had clinical representation. The Orthodontic pathway hadrepresentation from primary and community care GDPs, a primary care specialis<strong>to</strong>rthodontic practitioner and secondary care consultant Orthodontists. The OralSurgery pathway had clinical representation from primary care specialistpractitioners, secondary care oral surgeons and secondary care oral and maxillofacialsurgeons. Membership of <strong>the</strong>se groups can be found in Appendix three andfour.These national pathways represent a clinical consensus across NHSScotland. Theyhave been endorsed by <strong>the</strong> professional bodies: The Scottish OrthodonticConsultants’ Group and <strong>the</strong> Scottish Oral and Maxillo-Facial Society amongst o<strong>the</strong>rstakeholders. As a result, <strong>the</strong>re is already sign up and expectation for <strong>the</strong>irimplementation and embedding. The pathways should be tailored <strong>to</strong> accommodatelocal provision of <strong>the</strong>se services, and although <strong>the</strong> fundamental principles mustapply, local issues should be addressed accordingly. It was also found that key <strong>to</strong><strong>the</strong> success of delivering a pathway approach is likely <strong>to</strong> be <strong>the</strong> management ofpatient expectations.Action Planning - Implementing national pathwaysNHS Boards should ensure that <strong>the</strong> national pathways for Orthodontics and OralSurgery are promoted across both primary and secondary care and that <strong>the</strong>re isadherence <strong>to</strong> <strong>the</strong> thresholds for referral indicated. The pathways are attached asappendices Five and Six and may be accessed at:http://www.<strong>18</strong>weeks.scot.nhs.uk/how-<strong>to</strong>-achieve-and-maintain-<strong>18</strong>-weeks/patient-pathways/dentalspecialties/There may be fur<strong>the</strong>r scope for education and training. Targeted continuingprofessional development may assist GDPs in confidently applying referralpathways. There could be a role for National Education Scotland (NES) <strong>to</strong> develop awider programme of education.Index of Orthodontic <strong>Treatment</strong> NeedThe Index of Orthodontic <strong>Treatment</strong> Need (IOTN) is generally regarded as a helpful<strong>to</strong>ol in prioritising patients for referral and treatment <strong>to</strong> appropriate care providers i.e.specialist practitioners in primary care and clinicians in secondary care. IOTN usesboth an aes<strong>the</strong>tic and clinical component in order <strong>to</strong> assess an IOTN score, althougha higher IOTN score is not necessarily indicative of complexity of treatment required.Dental Specialties Task & Finish Group – January 2011 28
Initially it is expected that orthodontic colleagues will be <strong>the</strong> main user of IOTN and intime a uniform approach can be more widely applied.Action Planning - Index of Orthodontic <strong>Treatment</strong> NeedRaise awareness of IOTN and how it can be used in referral decisions by primarycare practitioners.Res<strong>to</strong>rative DentistryScottish Dental Needs Assessment ProgrammeA National project is underway within Res<strong>to</strong>rative Dentistry via <strong>the</strong> Scottish DentalNeeds Assessment Programme (SDNAP) and details of <strong>the</strong> remit of <strong>the</strong> project aredetailed below:AimTo conduct a needs assessment of specialist res<strong>to</strong>rative dentistry service provisionin all <strong>the</strong> Health Boards across Scotland and make recommendations.Objectives1. Study <strong>the</strong> current service delivery model in Scotland.2. Determine demand for <strong>the</strong> specialist res<strong>to</strong>rative service in NHS.3. Analyse workforce <strong>to</strong> support <strong>the</strong> current service model and potential servicemodels.4. Consider <strong>the</strong> cost of <strong>the</strong> current service model and potential service models.5. Determine perception of patients about <strong>the</strong> current service model.6. Determine perception of <strong>the</strong> service providers about <strong>the</strong> current servicemodel.7. Consider <strong>the</strong> current service model in <strong>the</strong> light of any Equality ImpactAssessment (EQIP)Progress <strong>to</strong> date• Completion of <strong>the</strong> current patient journey and current referral pathway (currentservice model), this will be explained in detail in <strong>the</strong> report along with quantitativedata.• As <strong>the</strong>re is no detailed data available <strong>to</strong> inform <strong>the</strong> report, SDNAP is conductingprospective data collection in all four dental hospitals. The data collected will helpinform <strong>the</strong> report and wider community about referral pro<strong>to</strong>cols, workforce, andDental Specialties Task & Finish Group – January 2011 29
implementation of <strong>18</strong> <strong>Weeks</strong> RTT <strong>Standard</strong>.• The pilot data collection was conducted in <strong>the</strong> first week of November 2010 atGlasgow Dental Hospital. The aim of <strong>the</strong> pilot was <strong>to</strong> test <strong>the</strong> feasibility of <strong>the</strong>data collection form and <strong>to</strong> make amendments, if need be. The data collectionform has been changed due <strong>to</strong> feedback received by <strong>the</strong> consultants. Actual datacollection will start in all <strong>the</strong> four Dental Hospitals i.e. Aberdeen Dental Hospital,Dundee Dental Hospital, Glasgow Dental Hospital, and Edinburgh Dental Instituteform 15 November <strong>to</strong> 10 December 2010 (four weeks). The data collection formwill completed by <strong>the</strong> res<strong>to</strong>rative consultant at <strong>the</strong> first out patient appointment forall <strong>the</strong> new patients. Margie Taylor (Chief Dental Officer) has kindly written letters<strong>to</strong> <strong>the</strong> four hospitals requesting that <strong>the</strong>y comply with data collection.• Almost completed: <strong>the</strong> in-depth interviews with res<strong>to</strong>rative consultantsabout <strong>the</strong>ir views about <strong>the</strong> service and also completed, a few interviewswith GDPs.• Undertaken four patient focus groups across Scotland based on <strong>the</strong>location i.e. urban, rural, remote etc.• Equality Impact Assessment has been done in conjunction with NHS QISand methodology followed is a literature search.• <strong>Report</strong> <strong>to</strong> be written (summer 2011).West of Scotland Dental Regional Planning GroupWest of Scotland NHS Boards are working <strong>to</strong>ge<strong>the</strong>r <strong>to</strong> develop a new regional modelof delivering res<strong>to</strong>rative dentistry. A linked aim is <strong>the</strong> desire <strong>to</strong> improve access <strong>to</strong> <strong>the</strong>service and enable referral <strong>to</strong> treatment standards <strong>to</strong> be met. This project is due <strong>to</strong>commence imminently and it is anticipated that <strong>the</strong> objectives will be <strong>to</strong> define a newservice model, gain regional agreement and implement regional standardised highvolume pathways.Managing Patient FlowsGiven long waits for treatment in certain dental specialties in a few areas, it is veryimportant <strong>to</strong> ensure that all lists are proactively managed, including validation ofpatients waiting and each patient’s actual need <strong>to</strong> be on a list.It is suggested that waiting lists can be managed more effectively by ensuring, forexample:• Effective booking systems are utilised• Treating patients in turn• Pooling listsDental Specialties Task & Finish Group – January 2011 30
• Managing DNA rates• Not listing patients until <strong>the</strong>y are ready for treatment• Referring for advice only• Managing return appointments differently <strong>to</strong> influence high new : return ratiosGoing back <strong>to</strong> basics and ensuring that good practice is firmly followed on a day <strong>to</strong>day basis may result in some fur<strong>the</strong>r quick wins in terms of maximising <strong>the</strong> use ofcapacity already available. Systems and processes should be continually reviewed<strong>to</strong> reduce bottlenecks and <strong>to</strong> allow smooth patient flows.Similarly, <strong>the</strong> use of <strong>the</strong> ‘what if’ analysis commended by <strong>the</strong> Orthopaedic ServicesTask and Finish Group, could be ano<strong>the</strong>r useful device <strong>to</strong> improving productivity byworking smarter, not harder. For fur<strong>the</strong>r information, please refer <strong>to</strong> <strong>the</strong>Orthopaedics Task and Finish output report pages 24 / 25:http://www.<strong>18</strong>weeks.scot.nhs.uk/how-<strong>to</strong>-achieve-and-maintain-<strong>18</strong>-weeks/task-andfinish-groups/orthopaedic-services/It is clearly recognised that much can be achieved by smoothing <strong>the</strong> hand-offs andreducing rate-limiting steps through all parts of <strong>the</strong> journey. Boards’ local <strong>18</strong> WeekTeams and Service Improvement Managers are skilled in applying <strong>the</strong>se conceptsand continue <strong>to</strong> provide fundamental guidance and support.Service Redesign and TransformationThe Task and Finish Group has close links with <strong>the</strong> national Improvement andSupport Team who offer direct support <strong>to</strong> NHS Boards, organising training anddevelopment <strong>to</strong> build capability and capacity for sustainable improvement.To support local visioning, pathway design and process improvement at <strong>the</strong> locallevel, <strong>the</strong> Task and Finish Group have sponsored ‘Key Areas <strong>to</strong> focus Improvement.’This is detailed in Appendix Two, and should be used as a device for planningservice redesign. Additionally in order <strong>to</strong> share <strong>the</strong> learning of o<strong>the</strong>r Board areas, a‘Who’s Doing What?’ matrix has been created, giving examples of work undertakenand contact details; this is detailed in Appendix Seven.Much of <strong>the</strong> key <strong>to</strong> success is about working smarter, not harder and about reevaluatingand updating key systems and processes.Action Planning - Service Redesign and TransformationEach Board should make best use of <strong>the</strong> service redesign methodologies andsupport available. This will help identify priority areas <strong>to</strong> focus improvement work.• The Task and Finish Group has explored opportunities <strong>to</strong> promote tele-dentistryacross Boards, particularly in remote and rural areas.Dental Specialties Task & Finish Group – January 2011 31
• Managed Clinical Networks <strong>to</strong> promote information sharing and developing andsharing good practice e.g. Tayside’s Orthodontic Managed Clinical Network.• Visioning days for Dentistry e.g. Forth Valley and Fife.• Consultants do not have <strong>to</strong> see all return patients; some patients could bereviewed by extended scope practitioners.• Increasing <strong>the</strong> number of ‘see and treat’ clinics.• Altered triage arrangements.• More regional working/services.For more examples of good practice, see <strong>the</strong> ‘Who is Doing What’ Matrix, attachedas Appendix seven.Tele-dentistryElectronic Orthodontics within <strong>the</strong> North of Scotland:Aspirations and Achievements <strong>to</strong> DateThe vision for <strong>the</strong> North of Scotland is <strong>to</strong> develop a common platform delivered onN3 <strong>to</strong> link Consultants working in hospital-based services, Primary Care DentalPractitioners, Information Services Division (ISD), <strong>the</strong> Scottish Dental Practice Board(SDPB), NHS Education Scotland and <strong>the</strong> North of Scotland’s Boards collaboratingin a Managed Clinical Network for Orthodontics. The overarching aim of <strong>the</strong> projectis <strong>to</strong> improve <strong>the</strong> quality of patient care by embracing technology, resulting in betteraccess <strong>to</strong> dental health information, ‘joined-up’ primary care and hospital servicesand quicker access <strong>to</strong> a unified dental record and imaging. However, it is not justabout technology, it is about modernising processes and encouraging new ways ofworking.Maximising existing and implementing new communication technologies <strong>to</strong> support<strong>the</strong> North of Scotland Managed Clinical Network (MCN) for Orthodontics is essential.Developing a system for information retrieval, collation and activity moni<strong>to</strong>ring will bea high priority for <strong>the</strong> MCN and is seen as fundamental <strong>to</strong> <strong>the</strong> Network’s success.A phased approach <strong>to</strong> implementation has been agreed. The capital required for ashort pilot (proof of concept) for Stage I and II was agreed by <strong>the</strong> North of ScotlandBoards.Stage I – Electronic Triage• Triage of orthodontic referrals sent by GDPs, Experienced Practitioners (SOP),Rural Fellows, etc, <strong>to</strong> a Consultant Orthodontist.• Preferred number of trial sites: five or six.• Functions required:o e-transfer of referral letter/form and response (s<strong>to</strong>re and forward);o ability <strong>to</strong> attach digital images (pho<strong>to</strong>graphs, PACS images), 3-D images, linksDental Specialties Task & Finish Group – January 2011 32
with CHI number, address book.• Information/Data Capture: Patient details including Date of Birth, address,referring clinician, demographics, etc.Timescale: Stage I has been completed.Stage II - <strong>Treatment</strong> Planning/Advice• <strong>Treatment</strong> Planning and Advice returned from a Consultant Orthodontist <strong>to</strong>experienced practitioners, rural fellows, GDPs etc.• Preferred number of trial sites: five or six.• Functions required: as for Stage I, and <strong>to</strong> include:o video conferencing/video assessment function;o recommendations/assessment report.• Information/Data Capture: As for Stage I, plus secure electronic patient recordwhich is accessible <strong>to</strong> Consultant, Dentist, AHP and o<strong>the</strong>r clinicians involved indirect patient dental care, as appropriate.Timescale: To be arranged.Stage III - Training and Education• E-Orthodontics will be evaluated as a <strong>to</strong>ol <strong>to</strong> support education and training atundergraduate and post graduate levels.• Interest in developing an MSc in e-Orthodontics has been expressed byProfessor James McDonald, Glasgow University.• It is envisaged that <strong>the</strong> e-orthodontics system will provide online help andtu<strong>to</strong>rials• Functionality required: as for I-III above, plus:o dictionary items;o on-line help screens;o full audit trail across <strong>the</strong> spectrum of treatment modalities, by referringpractice or discipline, financial aspects etc.Timescales: To be arranged.Stage IV - EDI in Primary Care• From Primary Care <strong>to</strong> ISD and <strong>the</strong> Scottish Dental Practice Board (SDPB)• Preferred number of trial sites: five or six• Function required: As for Stage I-III and <strong>to</strong> include:o Record of Services provided;o dental claim form <strong>to</strong> include authorisations required, etc.Ultimately, <strong>the</strong> intention is <strong>to</strong> utilise <strong>the</strong> NHS Scotland building blocks; N3, SCI S<strong>to</strong>re,Gateway and <strong>the</strong> Generic Clinical System <strong>to</strong> develop a multimedia, and multidisciplinarycare record from which <strong>the</strong> Information Statistics Division (ISD), <strong>the</strong>Scottish Dental Practice Board (SDPB) and <strong>the</strong> North of Scotland Managed ClinicalNetwork for Orthodontics will be able <strong>to</strong> access and exchange relevant information inorder <strong>to</strong> facilitate <strong>the</strong> commissioning, moni<strong>to</strong>ring and delivery of orthodontic care.Dental Specialties Task & Finish Group – January 2011 33
Robust evaluation will be carried out at <strong>the</strong> end of each stage. After which, <strong>the</strong>multimedia, and multi-disciplinary care record will be available <strong>to</strong> roll out <strong>to</strong> suppor<strong>to</strong><strong>the</strong>r NHS Boards and Orthodontic MCNs and link <strong>the</strong>m <strong>to</strong> a national Network.The multimedia and multi-disciplinary care record will be readily adaptable <strong>to</strong> meet<strong>the</strong> requirements of o<strong>the</strong>r emerging MCNs in dentistry.Dental Specialties’ Workforce Skills MixWorkforce considerations can inevitably impact on <strong>the</strong> ability of any service <strong>to</strong> delivertimely, high quality patient care.The Task and Finish Group clearly recognises recruitment difficulties faced in someNHS Boards. It is acknowledged that workforce issues in <strong>the</strong> central belt are quitedifferent <strong>to</strong> issues in, for example remote and rural areas, where a different range ofsolutions may be required. This, however, is even more reason <strong>to</strong> explore andaddress <strong>the</strong> skills mix and competency base within <strong>the</strong> existing workforce.NHS Boards are encouraged <strong>to</strong> review <strong>the</strong>ir workforce capacity and competencyprofile, with a view <strong>to</strong> streng<strong>the</strong>ning roles and responsibilities of differentcontribu<strong>to</strong>rs, <strong>to</strong> ensure that each task is undertaken by <strong>the</strong> most appropriate person.Increasing use of members of <strong>the</strong> multi disciplinary team, and development ofenhanced roles will free up considerable amounts of consultant time for direct patientcare. Given <strong>the</strong> existing multi-disciplinary workforce and <strong>the</strong> range of servicesprovided, many Boards have identified new ways of working <strong>to</strong> optimise <strong>the</strong> use ofand <strong>the</strong> skills-mix of available practitioners. This allows <strong>the</strong> development of existingcompetencies <strong>to</strong> support identified care pathways and streamline systems andprocessesIt is paramount for NHS Boards <strong>to</strong> have accurate activity data <strong>to</strong> ascertain workforcerequirements for each stage in <strong>the</strong> patient journey. Aspects of this approach form anelement of <strong>the</strong> Chief Dental Officer’s Workforce Review.Certain strategies could be adopted <strong>to</strong> assist with current workforce issues:• The role of <strong>the</strong> Dental Support Worker could be developed under pro<strong>to</strong>col, butthis would require additional education and training. This could be facilitated inconsultation with NHS Education Scotland.• Orthodontic Therapists are a new group of professionals who can assist with <strong>the</strong>clinical workload e.g. taking dental impressions and fitting brackets. Courses arecurrently available in Edinburgh and Coatbridge. There is also scope <strong>to</strong> use <strong>the</strong>seprofessionals’ in return Orthodontic appointments <strong>to</strong> free up consultants’ time fornew appointment slots.• There may be opportunities within secondary care <strong>to</strong> up-skill dentists inprocedures where <strong>the</strong>y may have previously lacked confidence, and <strong>the</strong>seprocedures can <strong>the</strong>refore be efficiently managed in <strong>the</strong> primary care setting.Dental Specialties Task & Finish Group – January 2011 34
Action Planning - WorkforceNHS Boards should review <strong>the</strong>ir workforce capacity and competency profile, with aview <strong>to</strong> streng<strong>the</strong>ning roles and responsibilities of different contribu<strong>to</strong>rs. Boardsshould make reference <strong>to</strong> <strong>the</strong> Chief Dental Officer’s Workforce Review <strong>to</strong> underpinworkforce planning assumptions and workforce development plans locally andnationally.Workforce Solutions WorkshopThis workshop <strong>to</strong>ok place in November 2009. A clear message from <strong>the</strong> day was <strong>to</strong>ensure that services are designed <strong>to</strong> meet patients’ needs and workforce planningneeds <strong>to</strong> support this key principle, which is also fundamental <strong>to</strong> sustainable deliveryof <strong>the</strong> <strong>18</strong> <strong>Weeks</strong> RTT <strong>Standard</strong>s. Principles that can assist with promoting thisconcept include:• Designing pathways <strong>to</strong> support <strong>the</strong> delivery of optimal care and patientexperience, and <strong>the</strong>se should be evidence based.• The design of a patient pathway should be used <strong>to</strong> determine <strong>the</strong> skills,competencies and roles required. The demand, and <strong>the</strong>refore capacity required,at each stage in <strong>the</strong> patient pathway needs <strong>to</strong> be quantified.• There should be an assessment of who does what at each stage in <strong>the</strong> pathway.There is evidence that professionals can be operating at <strong>the</strong> lower end of <strong>the</strong>ircompetency range, despite training and development. Workload and productivityshould be reviewed. This may provide some opportunities within current staffingfor increased capacity. Data from clinical outcoming may assist with this process.• Where new roles are developed <strong>the</strong>re is a need for standardisation of titles,responsibilities, skills and competencies and consideration of nationalaccreditation and validation.• More attention needs <strong>to</strong> be focused on administrative and clerical roles <strong>to</strong> supportpathway and patient flow management.All <strong>the</strong>se considerations should be used as a basis for informed workforce planning,both nationally and locally <strong>to</strong> facilitate provision of a workforce fit for <strong>the</strong> future, with asufficient number of dental undergraduates. Encouraging fur<strong>the</strong>r training of GDPsand a multi-skilled allied-professional workforce who are able <strong>to</strong> maximise <strong>the</strong>ircompetencies in providing high quality and timely dental care will contribute <strong>to</strong> <strong>the</strong>patient experience. However, <strong>the</strong>re is a need <strong>to</strong> focus on <strong>the</strong> initial management of<strong>the</strong> patient journey and what can be done in primary care <strong>to</strong> prevent <strong>the</strong> need foronward referral, especially if we are going <strong>to</strong> imbed <strong>the</strong> principles of Shifting <strong>the</strong>Balance of Care and delivering care closer <strong>to</strong> <strong>the</strong> patient’s home.Dental Specialties Task & Finish Group – January 2011 35
Action Planning - Specialist RolesNHS Boards <strong>to</strong> explore <strong>the</strong> scope for specialist roles and different ways of workingacross Dental Services. Evaluate skills mix and which professionals are best placed<strong>to</strong> undertake which functions. Where necessary this may be done under pro<strong>to</strong>col.Dental Specialties Task & Finish Group – January 2011 36
CommunicationStakeholder GroupsIn considering <strong>the</strong> issues for Dental Specialties and suitable methodologies fortackling <strong>the</strong> risks identified, care was taken by <strong>the</strong> Task and Finish Group <strong>to</strong> link asclosely as possible with key stakeholders (both individuals and groups), including:• North of Scotland Strategic Planning Group has co-ordinated considerations in<strong>the</strong> North and facilitated joint service planning, including <strong>the</strong> development ofcomprehensive action planning.• West of Scotland Dental Consortium• Chief Dental Officer’s Dental Lead Officers’ Meeting• Dental Stakeholders’ Group• Scottish Consultants’ Orthodontic Group• Scottish Oral and Maxillo-Facial Surgeons’ GroupNational EventsThe Improvement and Support Team hosted a series of national Dental Specialties’events on behalf of <strong>the</strong> Task and Finish Group, in order <strong>to</strong> engage with <strong>the</strong> dentalcommunity. Each provided an important forum for considering delivery expectations,sharing best practice and different approaches, and considering how NHSScotlandmight collectively overcome key bottlenecks (e.g. information ga<strong>the</strong>ring) in creating acritical path for delivery.Half day visioning events and Masterclasses <strong>to</strong>ok place which built on previousvisioning work. These event allowed colleagues <strong>to</strong> share good practice andfacilitated networking opportunities and collaborative working. A national DentalSpecialities event was held on <strong>the</strong> 25 March 2010.Action Planning - NetworkingAll Boards should continue <strong>to</strong> find ways <strong>to</strong> continue <strong>to</strong> network, linking withstakeholders across primary and secondary care <strong>to</strong> debate and deliver timely Dentalservices for <strong>the</strong> benefit of <strong>the</strong> patient.Dental Specialties Task & Finish Group – January 2011 37
Conclusion: Action Planning and Ongoing WorkThis Dental Specialties <strong>Output</strong> <strong>Report</strong> is intended <strong>to</strong> provide a blueprint for futureimprovement and delivery of dental services. Members of <strong>the</strong> Task and FinishGroup have focused in on <strong>the</strong> key issues which <strong>the</strong>y feel may have <strong>the</strong> maximumimpact. Each Board is now expected <strong>to</strong> use this <strong>to</strong> design a critical path for <strong>the</strong>unequivocal delivery of <strong>the</strong> <strong>18</strong> Week <strong>Referral</strong> <strong>to</strong> <strong>Treatment</strong> Target for dentalspecialties, and this report commends a series of key actions <strong>to</strong> Boards <strong>to</strong> underpinsuccessful delivery. Individual Boards will be performance managed through <strong>the</strong>coming months where delivery expectations are not being met.Some of <strong>the</strong> issues considered are easily implemented, leading <strong>to</strong> quick wins orearly gains e.g. ensuring <strong>the</strong> application of basic principles of waiting listmanagement. Some will be iterative in <strong>the</strong>ir application, and may needed <strong>to</strong> betested using <strong>the</strong> Plan-Do-Study-Act methodology <strong>to</strong> close <strong>the</strong> loop on improvementsproposed <strong>to</strong> allow optimum benefits. O<strong>the</strong>rs may rely on communication andembedding practice e.g. common application of definitions/ clock s<strong>to</strong>ps in order <strong>to</strong>accurately record a patient’s journey time. Much will be dependent on <strong>the</strong>organisation profile for <strong>the</strong>se services and <strong>the</strong> integration in<strong>to</strong> existing waiting timesstructures and delivery mechanisms. Individual Boards will be performance managedthrough <strong>the</strong> coming months if delivery proves elusive.The Task and Finish Group recognises and wishes <strong>to</strong> encourage scope for regionalapproaches <strong>to</strong> delivering timely dental services. The three Regional Offices haveeach given a high priority <strong>to</strong> <strong>the</strong>ir at risk dental specialties, and an ongoingcollaborative approach is being used <strong>to</strong> provide a focus on issues and solutionsacross each region. The North of Scotland Planning Group for example hasdeveloped a detailed action plan <strong>to</strong> address service shortfalls within dentistry.Dental Specialties Task & Finish Group – January 2011 38
Summary of Fundamental Next Steps for BoardsAction Planning – Points <strong>to</strong> ImplementMeasurementand Definitions• Ensure that generic <strong>18</strong> <strong>Weeks</strong> RTT definitions are applied <strong>to</strong>dental specialties at <strong>the</strong> highest level.• Use <strong>the</strong> bespoke FAQs and dental scenarios <strong>to</strong> ensure thatclock starts and s<strong>to</strong>ps are fully unders<strong>to</strong>od and universallyapplied.• Promote organisational learning and training on <strong>the</strong> applicationof <strong>the</strong>se definitions, especially among medical records,medical secretaries and clinic staff.• Pursue clinical outcome coding as <strong>the</strong> norm across all dentalspecialties.• Continue work <strong>to</strong> capture all treatment activity undertaken inan outpatient setting – especially in a return outpatient slot (notalways traditionally captured).• Promote <strong>the</strong> importance of accurate data capture andrecording across all dental specialties as a basis for serviceplanning, improvement and performance.• Ensure accurate, complete and validated Dental MonthlyManagement Information is returned <strong>to</strong> <strong>the</strong> ScottishGovernment and also used locally for management andimprovement).• Work with national stakeholders <strong>to</strong> improve data quality andcompleteness of national data returns, both for stage oftreatment (outpatients and inpatient/daycases) and wholeDemandCapacityActivity QueuePrimary CareSolutionsPerformanceManagementServiceRedesign andTransformationjourney <strong>18</strong> weeks measurement.• Use improved data sets as <strong>the</strong> basis for detailed capacitydemand planning for each of <strong>the</strong> dental specialties.• Use DCAQ <strong>to</strong>ols and methodologies <strong>to</strong> plan and optimise useof available slots.• Use QueSSTCap <strong>to</strong> predict and manage capacity gaps.• Pathway management.• Use professionally-developed and endorsed pathways <strong>to</strong>manage variations in referrals across practices, and <strong>to</strong>implement common thresholds for equity of access.• Drive uniform implementation and embedding of pathwaysacross <strong>the</strong> whole health community.• Promote and apply common referral thresholds fororthodontics (based on IOTN score).• When appropriate, request advice only treatment plan – thiswill not start an <strong>18</strong> Week RTT.• Use data <strong>to</strong> identify trends and risks and <strong>to</strong> manageperformance. Use ‘Key Areas <strong>to</strong> Focus Improvement’matrix <strong>to</strong>identify areas for fur<strong>the</strong>r work.• Use ‘who is doing what matrix’ <strong>to</strong> identify examples of goodpractice that can be transferred <strong>to</strong> your service.• Do not list patients until <strong>the</strong>y are suitable <strong>to</strong> commencetreatment.Dental Specialties Task & Finish Group – January 2011 39
• Analyse referral practices and consider teaching and practicalsessions for GDPs with routine procedures with which <strong>the</strong>ymay lack confidence.• Manage DNA rates e.g. text messaging reminders.• Promote, where appropriate ‘see and treat’ services.Cultural • Assure a high organisational profile for dental specialties.• Reinforce, culturally, that all Dental Specialties are part of <strong>18</strong>weeks RTT, including all treatments undertaken in anoutpatient setting.• Ensure strong high level leadership <strong>to</strong> support developments<strong>to</strong> secondary care dental services, with a strong culturalexpectation of delivery.Workforce • Review roles and competencies of dental specialties’ multidisciplinary teams• The design of a patient pathway should be used <strong>to</strong> determine<strong>the</strong> skills, competencies and roles required. The demand, and<strong>the</strong>refore capacity required, at each stage in <strong>the</strong> patientpathway needs <strong>to</strong> be quantified.• Consider increased use of enhanced roles (under pro<strong>to</strong>colwhere appropriate) <strong>to</strong> free up consultant time.• Use <strong>the</strong> Chief Dental Officer’s Workforce Review <strong>to</strong> underpinworkforce development plans locally and nationally.Communication • Sharing good practice e.g. via Managed Clinical Networks.• Consider adopting practices from <strong>the</strong> ‘Who is Doing What’matrix and liaising with Boards <strong>to</strong> ascertain best practices andhow <strong>to</strong> avoid pitfalls.Dental Specialties Task & Finish Group – January 2011 40
Appendix One: Membership of Dental Specialties Task and FinishGroupMemberDerek Leslie (chair)Board and RoleArgyll and Bute CHCP, General ManagerAlex Bowerman Scottish Government, Health Direc<strong>to</strong>rate,Programme Direc<strong>to</strong>rJacquie Dougall Scottish Government, Health Direc<strong>to</strong>rate, ProjectManagerMaura Edwards NHS Ayrshire and Arran, Consultant in DentalPublic HealthTom FerrisScottish Government, Deputy Chief Dental OfficerJanet HarrisKevin HillLaura JonesJim McDonaldRobert NaysmithHelen StrachanMargie TaylorScottish Government, Health Direc<strong>to</strong>rate, ServiceImprovement ManagerNHS Greater Glasgow and Clyde, Oral HealthDirec<strong>to</strong>rScottish Government, Health Direc<strong>to</strong>rate, NationalManager, <strong>18</strong> <strong>Weeks</strong> ProgrammeNHS Fife, Consultant OrthodontistNHS Lothian, Clinical Direc<strong>to</strong>r, Community andSalaried Dental ServiceNorth of Scotland, Regional Manager, Oral Healthand DentistryScottish Government, Chief Dental OfficerAppendix Two: Key Areas <strong>to</strong> Focus ImprovementSee diagram on next pageDental Specialties Task & Finish Group – January 2011 41
Dental Specialities Task & Finish GroupKey Areas <strong>to</strong> focus ImprovementDental Specialties have been highlighted across a number of NHS Boards as presenting a risk <strong>to</strong> delivery of <strong>18</strong> <strong>Weeks</strong> RTT.Orthodontics Oral Surgery Oral Medicine Res<strong>to</strong>rativePaediatricsGeneral Anaes<strong>the</strong>ticsThe NHS <strong>18</strong> weeks Service Redesign and Transformation Programme has developed a series of key changes which NHS Boards should considerwhen transforming services <strong>to</strong> improve <strong>the</strong> patient experience and <strong>to</strong> support delivery of <strong>18</strong> weeks RTT. These key changes focus on:• End <strong>to</strong> end planning of patient centred pathways delivered by <strong>the</strong> right person, at <strong>the</strong> right time, in <strong>the</strong> right care setting, ensuringquality at all times;• Working across organisational boundaries <strong>to</strong> utilise and develop <strong>the</strong> skills of <strong>the</strong> workforce <strong>to</strong> optimise clinical time <strong>to</strong> care;• Removal of waste and non-value adding steps and creation of flow;• Identifying, capturing and recording information flows which support and optimise both clinical and administrative processes.These key areas for improvement below are intended <strong>to</strong> provide a reference point <strong>to</strong> support organisations in ensuring service provision is being maximised fordental specialties in order <strong>to</strong> support delivery of a quality service, reduce patient waits and ensure patients are seen and treated in <strong>the</strong> appropriate care setting.REFERRAL• Understand referrals in<strong>to</strong> your service for alldental specialities and sub-specialities• Consider whe<strong>the</strong>r patients are placed on <strong>the</strong>appropriate pathway• Consider whe<strong>the</strong>r <strong>the</strong>re is potential foralternative management within generaldental practice ra<strong>the</strong>r than secondary care• Consider appropriateness of referrals withIOTN of
Appendix Three: Orthodontic <strong>Referral</strong> Management Pathway GroupNameMargie Taylor (chair)Joyce DalgleishJacquie DougallChristina HainingJanet HarrisDavid MorrantMark McCutcheonGrant McIntyreRobert NaysmithHelen StrachanBoard and RoleScottish Government, Chief Dental OfficerScottish Government, Health Direc<strong>to</strong>rate,Communications ManagerScottish Government, Health Direc<strong>to</strong>rate, ProjectManagerOrthodontist, Specialist Practitioner, Primary CareScottish Government, Health Direc<strong>to</strong>rate, SIMNHS Ayrshire and Arran, Consultant OrthodontistNHS Lothian, General Dental practitionerNHS Tayside, Consultant OrthodontistNHS Lothian, Clinical Direc<strong>to</strong>r, Community andSalaried Dental ServiceNorth of Scotland, Regional Manager, Oral Healthand DentistryDental Specialties Task & Finish Group – January 2011 43
Appendix Four: Oral Surgery <strong>Referral</strong> Management Pathway GroupNameMargie Taylor(chair)Roger CurrieHelen DevennieJoyce DalgleishJacquie DougallChristine GoodallMaura EdwardsTom FerrisJanet HarrisAndrew MeeVeronica MeeAvril NeilsonJulie SavinBoard and RoleScottish Government, Chief Dental OfficerNHS Ayrshire and Arran, Consultant Oral andMaxillofacial SurgeonNHS Highland, Oral Surgeon, Primary CareScottish Government, Health Direc<strong>to</strong>rate,Communications ManagerScottish Government, Health Direc<strong>to</strong>rate, ProjectManagerNHS Greater Glasgow and Clyde, Consultant OralSurgeonNHS Ayrshire and Arran, Consultant in Dental PublicHealthScottish Government, Deputy Chief Dental OfficerScottish Government, Health Direc<strong>to</strong>rate, SIMSpecialist Primary Care PractitionerSpecialist Primary Care PractitionerNHS Tayside, Consultant Oral SurgeonNHS Fife, Specialist Practitioner, Primary CareDental Specialties Task & Finish Group – January 2011 44
Appendix Five: Orthodontic Pathway and <strong>Referral</strong> GuidanceDental Specialties Task & Finish Group – January 2011 45
Dental Specialties Task & Finish Group – January 2011 46
Appendix Six: Oral Surgery Pathway and <strong>Referral</strong> GuidanceDental Specialties Task & Finish Group – January 2011 47
Dental Specialties Task & Finish Group – January 2011 48
Appendix Seven: Who is Doing What MatrixDental Specialties Task & Finish Group – January 2011 49

![Dr Matthew Checketts, NHS Tayside [PDF - 6Mb] - 18 Weeks](https://img.yumpu.com/49027155/1/190x143/dr-matthew-checketts-nhs-tayside-pdf-6mb-18-weeks.jpg?quality=85)


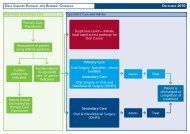
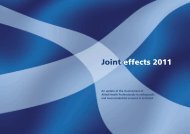


![Mark Sindall, NHS Dumfries and Galloway [PDF - 227Kb] - 18 Weeks](https://img.yumpu.com/30080335/1/190x143/mark-sindall-nhs-dumfries-and-galloway-pdf-227kb-18-weeks.jpg?quality=85)