

Delivering the 18 Weeks Referral to Treatment Standard Output Report
Delivering the 18 Weeks Referral to Treatment Standard Output Report
Delivering the 18 Weeks Referral to Treatment Standard Output Report

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
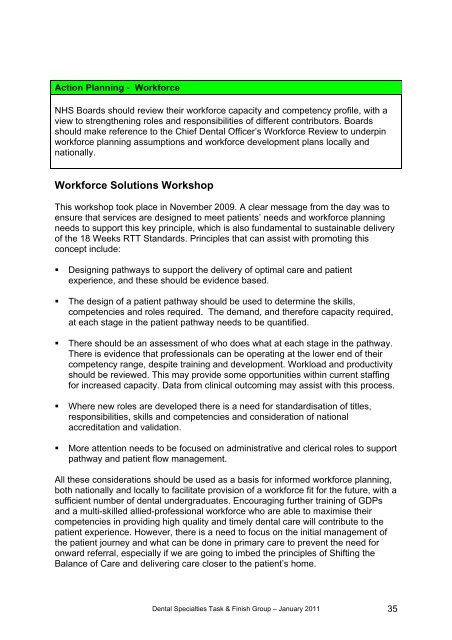
Action Planning - WorkforceNHS Boards should review <strong>the</strong>ir workforce capacity and competency profile, with aview <strong>to</strong> streng<strong>the</strong>ning roles and responsibilities of different contribu<strong>to</strong>rs. Boardsshould make reference <strong>to</strong> <strong>the</strong> Chief Dental Officer’s Workforce Review <strong>to</strong> underpinworkforce planning assumptions and workforce development plans locally andnationally.Workforce Solutions WorkshopThis workshop <strong>to</strong>ok place in November 2009. A clear message from <strong>the</strong> day was <strong>to</strong>ensure that services are designed <strong>to</strong> meet patients’ needs and workforce planningneeds <strong>to</strong> support this key principle, which is also fundamental <strong>to</strong> sustainable deliveryof <strong>the</strong> <strong>18</strong> <strong>Weeks</strong> RTT <strong>Standard</strong>s. Principles that can assist with promoting thisconcept include:• Designing pathways <strong>to</strong> support <strong>the</strong> delivery of optimal care and patientexperience, and <strong>the</strong>se should be evidence based.• The design of a patient pathway should be used <strong>to</strong> determine <strong>the</strong> skills,competencies and roles required. The demand, and <strong>the</strong>refore capacity required,at each stage in <strong>the</strong> patient pathway needs <strong>to</strong> be quantified.• There should be an assessment of who does what at each stage in <strong>the</strong> pathway.There is evidence that professionals can be operating at <strong>the</strong> lower end of <strong>the</strong>ircompetency range, despite training and development. Workload and productivityshould be reviewed. This may provide some opportunities within current staffingfor increased capacity. Data from clinical outcoming may assist with this process.• Where new roles are developed <strong>the</strong>re is a need for standardisation of titles,responsibilities, skills and competencies and consideration of nationalaccreditation and validation.• More attention needs <strong>to</strong> be focused on administrative and clerical roles <strong>to</strong> supportpathway and patient flow management.All <strong>the</strong>se considerations should be used as a basis for informed workforce planning,both nationally and locally <strong>to</strong> facilitate provision of a workforce fit for <strong>the</strong> future, with asufficient number of dental undergraduates. Encouraging fur<strong>the</strong>r training of GDPsand a multi-skilled allied-professional workforce who are able <strong>to</strong> maximise <strong>the</strong>ircompetencies in providing high quality and timely dental care will contribute <strong>to</strong> <strong>the</strong>patient experience. However, <strong>the</strong>re is a need <strong>to</strong> focus on <strong>the</strong> initial management of<strong>the</strong> patient journey and what can be done in primary care <strong>to</strong> prevent <strong>the</strong> need foronward referral, especially if we are going <strong>to</strong> imbed <strong>the</strong> principles of Shifting <strong>the</strong>Balance of Care and delivering care closer <strong>to</strong> <strong>the</strong> patient’s home.Dental Specialties Task & Finish Group – January 2011 35

![Dr Matthew Checketts, NHS Tayside [PDF - 6Mb] - 18 Weeks](https://img.yumpu.com/49027155/1/190x143/dr-matthew-checketts-nhs-tayside-pdf-6mb-18-weeks.jpg?quality=85)




![Mark Sindall, NHS Dumfries and Galloway [PDF - 227Kb] - 18 Weeks](https://img.yumpu.com/30080335/1/190x143/mark-sindall-nhs-dumfries-and-galloway-pdf-227kb-18-weeks.jpg?quality=85)