

Delivering the 18 Weeks Referral to Treatment Standard Output Report
Delivering the 18 Weeks Referral to Treatment Standard Output Report
Delivering the 18 Weeks Referral to Treatment Standard Output Report

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
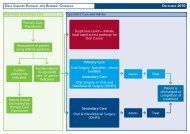
Influencing <strong>Referral</strong> ProcessesPart of <strong>the</strong> philosophy of NHSScotland is ensuring that each patient is seen by <strong>the</strong>right professional, in <strong>the</strong> right care setting, at <strong>the</strong> right time, first time. This maxim isparticularly relevant <strong>to</strong> dental specialties where a variety of patient pathways for <strong>the</strong>same condition have been witnessed. This may be addressed <strong>to</strong> a great extent byadopting standardised pathways as described in <strong>the</strong> section ‘Pathway Approach -Philosophy’, but also by influencing <strong>the</strong> referral process in<strong>to</strong> secondary care, with <strong>the</strong>patient right at <strong>the</strong> heart of this. It is <strong>the</strong>refore important <strong>to</strong> understand who iscoming in<strong>to</strong> secondary care, why are <strong>the</strong>y coming in, is this <strong>the</strong> best place for <strong>the</strong>patient <strong>to</strong> be, and what are <strong>the</strong> influencing fac<strong>to</strong>rs for each referral?Demand is not a givenIt has been suggested that a high proportion of patients are assessed and treated in<strong>the</strong> wrong care setting.In 2007-2008 approximately 45% of oral surgery procedures performed in one NHSBoard were coded as ‘simple’ extraction of <strong>to</strong>oth. Simple extractions can beperformed in <strong>the</strong> primary/community care setting which would reduce demand onhospital services.Simple extractions are often referred <strong>to</strong> oral surgery departments within secondarycare, as some General Dental Practitioners (GDPs) refer in, choosing not <strong>to</strong>undertake this procedure <strong>the</strong>mselves. Variation in service supply in different parts of<strong>the</strong> country and <strong>the</strong> impact that this may have upon models of care within differen<strong>the</strong>alth communities has already been recognised. However, <strong>the</strong>re remains scope fordeveloping a clearer understanding of referral patterns by practice, along withvariation in rates of referral for different dental conditions. The outputs of this workcould be used locally <strong>to</strong>:• Develop referral thresholds, which should usefully be linked <strong>to</strong> clinical standardsabout where thresholds lie.• Influence <strong>the</strong> type and <strong>the</strong> quality of referrals e.g. tick box stationery.• Explore <strong>the</strong> scope for increased continuing professional development, educationand training <strong>to</strong> overcome recurrent referrals in specific areas.• Feedback <strong>to</strong> origina<strong>to</strong>rs regarding <strong>the</strong> quality of referrals and data regarding <strong>the</strong>purpose and timeliness of referrals.• Discuss different referral patterns with outlying practices <strong>to</strong> consider alternativeapproaches.This is occurring in o<strong>the</strong>r clinical specialties and is <strong>the</strong> subject of one of <strong>the</strong>workstreams of <strong>the</strong> Capacity / Demand Management Task and Finish Group. It hasDental Specialties Task & Finish Group – January 2011 24

![Dr Matthew Checketts, NHS Tayside [PDF - 6Mb] - 18 Weeks](https://img.yumpu.com/49027155/1/190x143/dr-matthew-checketts-nhs-tayside-pdf-6mb-18-weeks.jpg?quality=85)




![Mark Sindall, NHS Dumfries and Galloway [PDF - 227Kb] - 18 Weeks](https://img.yumpu.com/30080335/1/190x143/mark-sindall-nhs-dumfries-and-galloway-pdf-227kb-18-weeks.jpg?quality=85)