

Netherlands Journal
NJCC Volume 10, Oktober 2006
NJCC Volume 10, Oktober 2006
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
netherlands journal of critical care<br />
Table 1. results of microscopy and culture for A. fumigatus<br />
Day in ICU Sample Method / Result<br />
14 BAL Microscopy: hyphae<br />
Culture: A. fumigatus<br />
15 Sputum Microscopy: hyphae<br />
Culture: A. fumigatus<br />
20 Sputum Microscopy: no hyphae<br />
Culture: A. fumigatus<br />
23 BAL<br />
Biopsy<br />
Microscopy: no hyphae<br />
Culture: A. fumigatus<br />
Microscopy: hyphae<br />
Culture: A. fumigatus<br />
44 Sputum Microscopy: no hyphae<br />
Culture: A. fumigatus<br />
BAL = bronchoalveolar lavage fluid.<br />
a temporary acquired immunodeficiency, facilitating opportunistic<br />
infections to develop in apparently immunocompetent patients [2].<br />
Conditions like, chronic lung disease, non-haematological malignancy,<br />
HIV infection, diabetes mellitus, liver failure, chronic alcohol<br />
abuse, malnutrition and extensive burns have been reported in<br />
association with invasive aspergillosis [8] and the interpretation of<br />
finding ubiquitous, branched hyphae in a culture taken from a nonsterile<br />
site remains difficult. In the absence of large epidemiological<br />
studies there are no known risk factors, single or in combination, for<br />
the acquisition of an invasive Aspergillus infection. Polymerase chain<br />
reaction (PCR) allows detection of the equivalent of 10-100 colonyforming<br />
units (CFU) of Aspergillus fumigatus per sample in serum or<br />
plasma. The combined use of PCR for A. fumigatus DNA and ELISA<br />
for galactomannan should provide a definitive diagnosis of invasive<br />
aspergillosis, even in the absence of obvious clinical signs [9]. As<br />
long as these methods are not generally available, direct microscopic<br />
examination of BAL fluid remains the first and most important clue<br />
to a potentially lethal mycosis. Retrospectively, there were no known<br />
predisposing factors for invasive aspergillosis or indications of reduced<br />
pulmonary host defences in our patient other than sepsis. For<br />
immunocompromised patients with cancer and hematopoietic stem<br />
cell transplants definitions of invasive fungal infections and the best<br />
methods for establishing the diagnosis are published as an international<br />
consensus [10]. However regarding immune competent hosts<br />
there remains much uncertainty. A diagnostic algorithm for patients<br />
without a malignancy as proposed by van de Woude et al. [8] should<br />
trigger physicians not to take a culture containing Aspergillus spp. too<br />
easily for contamination.<br />
Figure 1, CT scan of the thorax showing infiltrative abnormalities, mainly in the right upper<br />
lobe, and pleural effusion. No cavities were found.<br />
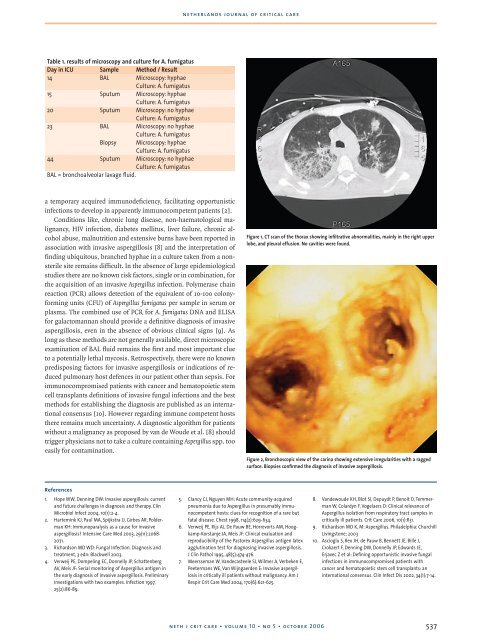
Figure 2, Bronchoscopic view of the carina showing extensive irregularities with a ragged<br />
surface. Biopsies confirmed the diagnosis of invasive aspergillosis.<br />
References<br />
1. Hope WW, Denning DW: Invasive aspergillosis: current<br />
and future challenges in diagnosis and therapy. Clin<br />
Microbiol Infect 2004, 10(1):2-4.<br />
2. Hartemink KJ, Paul MA, Spijkstra JJ, Girbes AR, Polderman<br />
KH: Immunoparalysis as a cause for invasive<br />
aspergillosis? Intensive Care Med 2003, 29(11):2068-<br />
2071.<br />
3. Richardson MD WD: Fungal Infection. Diagnosis and<br />
treatment, 3 edn: Blackwell 2003.<br />
4. Verweij PE, Dompeling EC, Donnelly JP, Schattenberg<br />
AV, Meis JF: Serial monitoring of Aspergillus antigen in<br />
the early diagnosis of invasive aspergillosis. Preliminary<br />
investigations with two examples. Infection 1997,<br />
25(2):86-89.<br />
5. Clancy CJ, Nguyen MH: Acute community-acquired<br />
pneumonia due to Aspergillus in presumably immunocompetent<br />
hosts: clues for recognition of a rare but<br />
fatal disease. Chest 1998, 114(2):629-634.<br />
6. Verweij PE, Rijs AJ, De Pauw BE, Horrevorts AM, Hoogkamp-Korstanje<br />
JA, Meis JF: Clinical evaluation and<br />
reproducibility of the Pastorex Aspergillus antigen latex<br />
agglutination test for diagnosing invasive aspergillosis.<br />
J Clin Pathol 1995, 48(5):474-476.<br />
7. Meersseman W, Vandecasteele SJ, Wilmer A, Verbeken E,<br />
Peetermans WE, Van Wijngaerden E: Invasive aspergillosis<br />
in critically ill patients without malignancy. Am J<br />
Respir Crit Care Med 2004, 170(6):621-625.<br />
8. Vandewoude KH, Blot SI, Depuydt P, Benoit D, Temmerman<br />
W, Colardyn F, Vogelaers D: Clinical relevance of<br />
Aspergillus isolation from respiratory tract samples in<br />
critically ill patients. Crit Care 2006, 10(1):R31.<br />
9. Richardson MD K, M: Aspergillus. Philadelphia: Churchill<br />
Livingstone; 2003<br />
10. Ascioglu S, Rex JH, de Pauw B, Bennett JE, Bille J,<br />
Crokaert F, Denning DW, Donnelly JP, Edwards JE,<br />
Erjavec Z et al: Defining opportunistic invasive fungal<br />
infections in immunocompromised patients with<br />
cancer and hematopoietic stem cell transplants: an<br />
international consensus. Clin Infect Dis 2002, 34(1):7-14.<br />
neth j crit care • volume 10 • no 5 • october 2006<br />
537




