

Netherlands Journal
NJCC Volume 10, Oktober 2006
NJCC Volume 10, Oktober 2006
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
netherlands journal of critical care<br />
Copyright ©2006, Nederlandse Vereniging voor Intensive Care. All Rights Reserved. Received August 2006; accepted in revised form September 2006<br />
c l i n i c a l i m a g e<br />
Incomplete circle of Willis<br />
H.R.H. de Geus, J. Bakker<br />
Department of Intensive Care, Erasmus University Medical Centre Rotterdam, The <strong>Netherlands</strong><br />
Abstract. A 60-year-old woman presented with acute headache and loss of consciousness. On admission her Glasgow coma<br />
scale score was 6. She was intubated in order to secure the airway. The computer tomography scan (CT-scan) showed a huge<br />
amount of subarachnoidal blood probably due to an aneurysmal haemorrhage. Further CT-angiography and image reconstruction<br />
identified the aneurysm as being situated in the anterior communicating artery (Figure 1). Furthermore there was an incomplete<br />
circulus arteriosus cerebri (circle of Willis) with an absent posterior communicating artery on both sides and the right anterior<br />
cerebral artery originating in the left carotid artery with absence of communication between the right anterior cerebral artery and<br />
the right middle cerebral artery. There were no neurosurgical or endovascular treatment options. Despite optimal management<br />
by preventing vasospasm with excessive fluid infusion, calcium channel blockers and dobutamine she developed frontal lobe<br />
ischaemia (Figure 2) and cardiac failure with acute pulmonary oedema. After a fulminant re-bleed our patient was brain-dead and<br />
further medical treatment was discontinued.<br />
Merkkola et al studied 87 post-mortem patients identifying missing posterior communicating arteries in 46% and missing or incomplete<br />
anterior communicating arteries in 22%. (1) The developmental absence of both communicating systems is rare and proved<br />
fatal in this case of subarachnoidal haemorrhage. Because of the high risk of ischaemia during neurosurgical or endovascular intervention<br />
the treatment of the aneurysm in these cases is suboptimal, thus increasing the risk of a fatal re-bleed.<br />
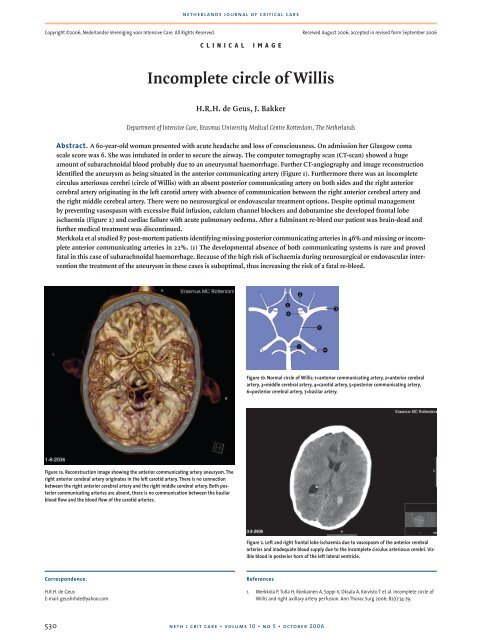
Figure 1b. Normal circle of Willis; 1=anterior communicating artery, 2=anterior cerebral<br />
artery, 3=middle cerebral artery, 4=carotid artery, 5=posterior communicating artery,<br />
6=posterior cerebral artery, 7=basilar artery.<br />
Figure 1a. Reconstruction image showing the anterior communicating artery aneurysm. The<br />
right anterior cerebral artery originates in the left carotid artery. There is no connection<br />
between the right anterior cerebral artery and the right middle cerebral artery. Both posterior<br />
communicating arteries are absent, there is no communication between the basilar<br />
blood flow and the blood flow of the carotid arteries.<br />
Figure 2. Left and right frontal lobe ischaemia due to vasospasm of the anterior cerebral<br />
arteries and inadequate blood supply due to the incomplete circulus arteriosus cerebri. Visible<br />
blood in posterior horn of the left lateral ventricle.<br />
Correspondence:<br />
H.R.H. de Geus<br />
E-mail: geushrhde@yahoo.com<br />
References<br />
1. Merkkola P, Tulla H, Ronkainen A, Soppi V, Oksala A, Koivisto T et al. Incomplete circle of<br />
Willis and right axillary artery perfusion. Ann Thorac Surg 2006; 82(1):74-79.<br />
530<br />
neth j crit care • volume 10 • no 5 • october 2006




