

VA/DoD CLINICAL PRACTICE GUIDELINE FOR OPIOID THERAPY FOR CHRONIC PAIN
2lfFhbO
2lfFhbO

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>VA</strong>/<strong>DoD</strong> Clinical Practice Guideline for Opioid Therapy for Chronic Pain<br />
2010<br />
Recommendation<br />
Location 18 2010 Recommendation Text 19<br />
Module<br />
Section<br />
Number<br />
signatures<br />
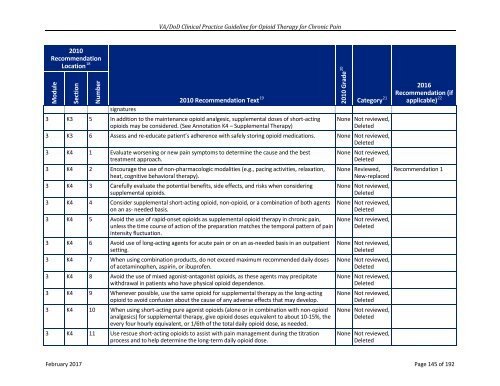
3 K3 5 In addition to the maintenance opioid analgesic, supplemental doses of short-acting<br />
opioids may be considered. (See Annotation K4 – Supplemental Therapy)<br />
2010 Grade 20<br />
2016<br />
Recommendation (if<br />
Category 21 applicable) 22<br />
None Not reviewed,<br />
Deleted<br />
3 K3 6 Assess and re-educate patient’s adherence with safely storing opioid medications. None Not reviewed,<br />
Deleted<br />
3 K4 1 Evaluate worsening or new pain symptoms to determine the cause and the best<br />
treatment approach.<br />
3 K4 2 Encourage the use of non-pharmacologic modalities (e.g., pacing activities, relaxation,<br />
heat, cognitive behavioral therapy).<br />
3 K4 3 Carefully evaluate the potential benefits, side effects, and risks when considering<br />
supplemental opioids.<br />
3 K4 4 Consider supplemental short-acting opioid, non-opioid, or a combination of both agents<br />
on an as- needed basis.<br />
3 K4 5 Avoid the use of rapid-onset opioids as supplemental opioid therapy in chronic pain,<br />
unless the time course of action of the preparation matches the temporal pattern of pain<br />
intensity fluctuation.<br />
3 K4 6 Avoid use of long-acting agents for acute pain or on an as-needed basis in an outpatient<br />
setting.<br />
3 K4 7 When using combination products, do not exceed maximum recommended daily doses<br />
of acetaminophen, aspirin, or ibuprofen.<br />
3 K4 8 Avoid the use of mixed agonist-antagonist opioids, as these agents may precipitate<br />
withdrawal in patients who have physical opioid dependence.<br />
3 K4 9 Whenever possible, use the same opioid for supplemental therapy as the long-acting<br />
opioid to avoid confusion about the cause of any adverse effects that may develop.<br />
3 K4 10 When using short-acting pure agonist opioids (alone or in combination with non-opioid<br />
analgesics) for supplemental therapy, give opioid doses equivalent to about 10-15%, the<br />
every four hourly equivalent, or 1/6th of the total daily opioid dose, as needed.<br />
3 K4 11 Use rescue short-acting opioids to assist with pain management during the titration<br />
process and to help determine the long-term daily opioid dose.<br />
None Not reviewed,<br />
Deleted<br />
None Reviewed,<br />
New-replaced<br />
None Not reviewed,<br />
Deleted<br />
None Not reviewed,<br />
Deleted<br />
None Not reviewed,<br />
Deleted<br />
None Not reviewed,<br />
Deleted<br />
None Not reviewed,<br />
Deleted<br />
None Not reviewed,<br />
Deleted<br />
None Not reviewed,<br />
Deleted<br />
None Not reviewed,<br />
Deleted<br />
None Not reviewed,<br />
Deleted<br />
Recommendation 1<br />
February 2017 Page 145 of 192