

VA/DoD CLINICAL PRACTICE GUIDELINE FOR OPIOID THERAPY FOR CHRONIC PAIN
2lfFhbO
2lfFhbO

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
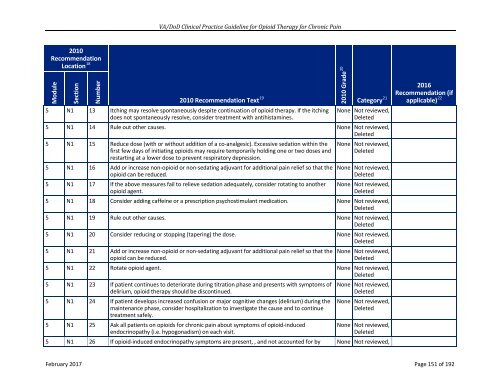
<strong>VA</strong>/<strong>DoD</strong> Clinical Practice Guideline for Opioid Therapy for Chronic Pain<br />
2010<br />
Recommendation<br />
Location 18 2010 Recommendation Text 19<br />
Module<br />
Section<br />
Number<br />
5 N1 13 Itching may resolve spontaneously despite continuation of opioid therapy. If the itching<br />
does not spontaneously resolve, consider treatment with antihistamines.<br />
5 N1 14 Rule out other causes. None Not reviewed,<br />
Deleted<br />
5 N1 15 Reduce dose (with or without addition of a co-analgesic). Excessive sedation within the<br />
first few days of initiating opioids may require temporarily holding one or two doses and<br />
restarting at a lower dose to prevent respiratory depression.<br />
5 N1 16 Add or increase non-opioid or non-sedating adjuvant for additional pain relief so that the<br />
opioid can be reduced.<br />
5 N1 17 If the above measures fail to relieve sedation adequately, consider rotating to another<br />
opioid agent.<br />
2010 Grade 20<br />
2016<br />
Recommendation (if<br />
Category 21 applicable) 22<br />
None Not reviewed,<br />
Deleted<br />
None Not reviewed,<br />
Deleted<br />
None Not reviewed,<br />
Deleted<br />
None Not reviewed,<br />
Deleted<br />
5 N1 18 Consider adding caffeine or a prescription psychostimulant medication. None Not reviewed,<br />
Deleted<br />
5 N1 19 Rule out other causes. None Not reviewed,<br />
Deleted<br />
5 N1 20 Consider reducing or stopping (tapering) the dose. None Not reviewed,<br />
Deleted<br />
5 N1 21 Add or increase non-opioid or non-sedating adjuvant for additional pain relief so that the<br />
opioid can be reduced.<br />
None Not reviewed,<br />
Deleted<br />
5 N1 22 Rotate opioid agent. None Not reviewed,<br />
Deleted<br />
5 N1 23 If patient continues to deteriorate during titration phase and presents with symptoms of<br />
delirium, opioid therapy should be discontinued.<br />
5 N1 24 If patient develops increased confusion or major cognitive changes (delirium) during the<br />
maintenance phase, consider hospitalization to investigate the cause and to continue<br />
treatment safely.<br />
5 N1 25 Ask all patients on opioids for chronic pain about symptoms of opioid-induced<br />
endocrinopathy (i.e. hypogonadism) on each visit.<br />
None Not reviewed,<br />
Deleted<br />
None Not reviewed,<br />
Deleted<br />
None Not reviewed,<br />
Deleted<br />
5 N1 26 If opioid-induced endocrinopathy symptoms are present, , and not accounted for by None Not reviewed,<br />
February 2017 Page 151 of 192