

RHM Pension Plan 35 and Plan 45 - RHM Pension Scheme - UK.com
RHM Pension Plan 35 and Plan 45 - RHM Pension Scheme - UK.com
RHM Pension Plan 35 and Plan 45 - RHM Pension Scheme - UK.com

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
◆<br />
42<br />
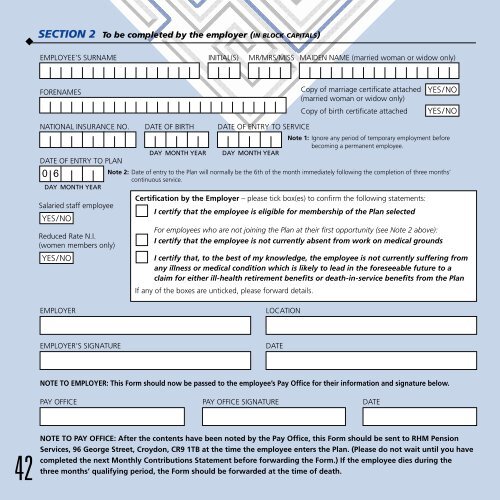
SECTION 2 To be <strong>com</strong>pleted by the employer (IN BLOCK CAPITALS)<br />
EMPLOYEE’S SURNAME INITIAL(S) MR/MRS/MISS MAIDEN NAME (married woman or widow only)<br />
FORENAMES<br />
Reduced Rate N.I.<br />
(women members only)<br />
YES/NO<br />
EMPLOYER LOCATION<br />
EMPLOYER’S SIGNATURE DATE<br />
Copy of marriage certificate attached<br />
(married woman or widow only)<br />
Copy of birth certificate attached<br />
YES/NO<br />
YES/NO<br />
NATIONAL INSURANCE NO. DATE OF BIRTH DATE OF ENTRY TO SERVICE<br />
Note 1: Ignore any period of temporary employment before<br />
be<strong>com</strong>ing a permanent employee.<br />
DATE OF ENTRY TO PLAN<br />
DAY MONTH YEAR DAY MONTH YEAR<br />
0 6<br />
DAY MONTH YEAR<br />
Note 2: Date of entry to the <strong>Plan</strong> will normally be the 6th of the month immediately following the <strong>com</strong>pletion of three months’<br />
continuous service.<br />
Certification by the Employer – please tick box(es) to confirm the following statements:<br />
Salaried staff employee<br />
YES/NO<br />
I certify that the employee is eligible for membership of the <strong>Plan</strong> selected<br />
For employees who are not joining the <strong>Plan</strong> at their first opportunity (see Note 2 above):<br />
I certify that the employee is not currently absent from work on medical grounds<br />
I certify that, to the best of my knowledge, the employee is not currently suffering from<br />
any illness or medical condition which is likely to lead in the foreseeable future to a<br />
claim for either ill-health retirement benefits or death-in-service benefits from the <strong>Plan</strong><br />
If any of the boxes are unticked, please forward details.<br />
NOTE TO EMPLOYER: This Form should now be passed to the employee’s Pay Office for their information <strong>and</strong> signature below.<br />
PAY OFFICE PAY OFFICE SIGNATURE DATE<br />
NOTE TO PAY OFFICE: After the contents have been noted by the Pay Office, this Form should be sent to <strong>RHM</strong> <strong>Pension</strong><br />
Services, 96 George Street, Croydon, CR9 1TB at the time the employee enters the <strong>Plan</strong>. (Please do not wait until you have<br />
<strong>com</strong>pleted the next Monthly Contributions Statement before forwarding the Form.) If the employee dies during the<br />
three months’ qualifying period, the Form should be forwarded at the time of death.