SMD PRESENTATION - longue vie et autonomie (HEGP)
SMD PRESENTATION - longue vie et autonomie (HEGP)
SMD PRESENTATION - longue vie et autonomie (HEGP)

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
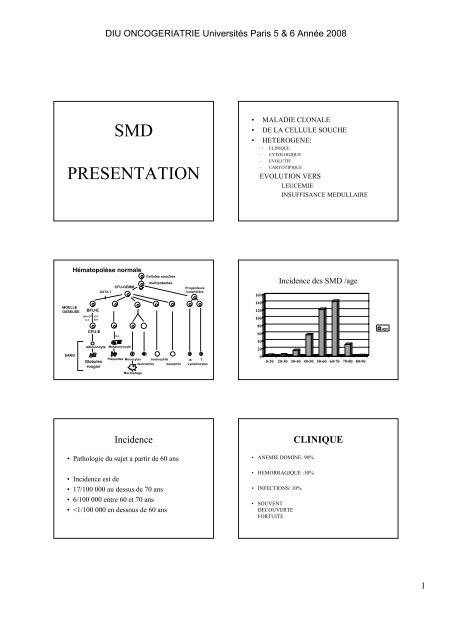
DIU ONCOGERIATRIE Universités Paris 5 & 6 Année 2008<br />
<strong>SMD</strong><br />
<strong>PRESENTATION</strong><br />
• MALADIE CLONALE<br />
• DE LA CELLULE SOUCHE<br />
• HETEROGENE:<br />
- CLINIQUE<br />
– CYTOLOGIQUE<br />
– EVOLUTIF<br />
– CARYOTIPIQUE<br />
EVOLUTION VERS<br />
LEUCEMIE<br />
INSUFFISANCE MEDULLAIRE<br />
Hématopoïèse normale<br />
GATA-1<br />
CFU-GEMM<br />
Cellules souches<br />
multipotentes<br />
Progéniteurs<br />
lymphoïdes<br />
160<br />
Incidence des <strong>SMD</strong> /age<br />
MOELLE<br />
OSSEUSE<br />
GM-SCF<br />
IL-3<br />
BFU-E<br />
SCF<br />
Epo<br />
140<br />
120<br />
100<br />
SANG<br />
CFU-E<br />
réticulocyte Mégacaryocyte<br />
Globules<br />
rouges<br />
Tpo<br />
Plaqu<strong>et</strong>tes Monocytes éosinophile<br />
neutrophile basophile<br />
B T<br />
Lymphocytes<br />
80<br />
60<br />
40<br />
20<br />
0<br />
0-20 20-30 30-40 40-50 50-60 60-70 70-80 80-90<br />
age<br />
Macrophage<br />
Incidence<br />
CLINIQUE<br />
• Pathologie du suj<strong>et</strong> a partir de 60 ans<br />
• Incidence est de<br />
• 17/100 000 au dessus de 70 ans<br />
• 6/100 000 entre 60 <strong>et</strong> 70 ans<br />
•
DIU ONCOGERIATRIE Universités Paris 5 & 6 Année 2008<br />
CLINIQUE<br />
ANEMIE<br />
• SPLENOMEGALIE<br />
AR<br />
LMMC<br />
FIBROSE<br />
• LOCALISATIONS CUTANEES<br />
LOCALISATIONS SPECIFIQUES DES LMMC<br />
VASCULARITES A NEUTROPHILES<br />
SYNDROME DE SWEET<br />
ACRA ERYTHEMA<br />
• PRESENTE DANS 90%<br />
DES CAS<br />
• NORMOCYTAIRE OU<br />
MACROCYTAIRE<br />
• NON REGENERATIVE<br />
• EVOLUTION LENTE<br />
Hb normale:13%<br />
normal Hb level<br />
13%<br />
abnormal Hb level<br />
87%<br />
Hb>=10 g/dL<br />
37%<br />
Hb
DIU ONCOGERIATRIE Universités Paris 5 & 6 Année 2008<br />
Polychondrite atrophiante <strong>et</strong><br />
<strong>SMD</strong><br />
Polychondrite atrophiante <strong>et</strong><br />
<strong>SMD</strong><br />
MDS ET SWEET<br />
<strong>SMD</strong> <strong>et</strong> Polyarthrites<br />
Étiologies<br />
Anti-mitotiques<br />
• 36% des <strong>SMD</strong><br />
– Anti-mitotiques<br />
– Toxiques<br />
– Radiations ionisantes<br />
– Hémopathies acquises<br />
– Pathologies<br />
congénitales<br />
Exposition à des<br />
toxiques<br />
36%<br />
10% Pesticides/Herbicides/<br />
5% Engrais<br />
8%<br />
Poussières minérales<br />
11%<br />
10%<br />
Métaux<br />
56%<br />
Hydrocarbures<br />
Solvants<br />
Tabac<br />
Aucune exposition<br />
64%<br />
• Alkylants ++ : melphalan <strong>et</strong> moutardes d’azote<br />
‣ dose dépendant, terrain <strong>et</strong> pathologie sous-jacente<br />
‣ max à 5-8 ans, quasi nulle après 10 ans<br />
• Anti-métabolites : Hydréa <strong>et</strong> Vercyte<br />
‣ TE <strong>et</strong> PV : 3% <strong>et</strong> 10-20 de <strong>SMD</strong> <strong>et</strong> LAM<br />
‣ +++ si association<br />
• Immunosuppresseurs : Aziathioprine,Endoxan<br />
‣ Dose dépendant / selon le polymorphisme de<br />
métabolisme du médicament<br />
• Fludarabine : ++ en association<br />
3
DIU ONCOGERIATRIE Universités Paris 5 & 6 Année 2008<br />
Toxiques<br />
• Benzène : industrie +++, tabagisme<br />
max 8-10 ans,<br />
cytogénétiques récurrentes : del 5, del 7<br />
polymorphisme génétique enzymes du<br />
métabolisme du benzène<br />
• Hydrocarbures, Solvants, Pesticides<br />
Radiations ionisantes<br />
• Incidence ++ 10ans après Hiroshima <strong>et</strong><br />
Nagasaki<br />
• Radiothérapie : ++ si champ large <strong>et</strong> age<br />
>40 ans /modèle de la maladie de Hodgkin<br />
• Pas incidence des autres rayonnements<br />
Études<br />
West 1995<br />
Mele 1994<br />
Ido1996<br />
Pasqual<strong>et</strong>ti1997<br />
Rigolin1998<br />
Nagata1999<br />
Bjork 2000<br />
Agents environnementaux<br />
Tabac<br />
1.16<br />
P100 cas)<br />
Laque<br />
2.38 peroxydes<br />
1.5<br />
1.77<br />
NA<br />
NA<br />
1.99<br />
NA<br />
Alcool<br />
NA<br />
NA<br />
P
DIU ONCOGERIATRIE Universités Paris 5 & 6 Année 2008<br />
Classification FAB<br />
SURVIE SELON LA FAB<br />
AR<br />
Blastes sg<br />
%<br />
< 1%<br />
Blastes<br />
moelle %<br />
< 5%<br />
Sidéroblastes<br />
moelle<br />
15%<br />
AREB<br />
< 5%<br />
5-20%<br />
5%<br />
20-30%<br />
DIU ONCOGERIATRIE Universités Paris 5 & 6 Année 2008<br />
Problèmes de la classification<br />
• Anomalies<br />
cytogénétiques<br />
• Transfusion est un<br />
facteur pronostique<br />
Cumulative proportion surviving<br />
1.0<br />
0.9<br />
0.8<br />
0.7<br />
0.6<br />
0.5<br />
0.4<br />
0.3<br />
0.2<br />
0.1<br />
0.0<br />
Survival of MDS patients according to<br />
transfusion dependency<br />
Overall survival<br />
(HR = 1.91, p < 0.001)<br />
Transfusion-independent<br />
Transfusion-dependent<br />
0 20 40 60 80 100 120 140 160 180<br />
Survival time (months)<br />
Cumulative proportion surviving<br />
1.0<br />
0.9<br />
0.8<br />
0.7<br />
0.6<br />
0.5<br />
0.4<br />
0.3<br />
0.2<br />
0.1<br />
Leukaemia-free survival<br />
(HR = 1.84, p = 0.001)<br />
Transfusion-independent<br />
Transfusion-dependent<br />
0.0<br />
0 20 40 60 80 100 120 140 160 180<br />
Survival time (months)<br />
Malcovati L, <strong>et</strong> al. J Clin Oncol. 2005;23:7594-603.<br />
Anomalies cytogénétiques<br />
Anomalies cytogénétiques<br />
• Le nombre<br />
d’anomalies est un<br />
facteur péjoratif<br />
• Plusieurs groupes:<br />
• Good risk:<br />
Normaux;20q ;5q<br />
• Int -1:Trisomie 8<br />
• Int-2 -7;7q;Complexes<br />
non 5 <strong>et</strong> 7<br />
• High: Complexes 5,7<br />
Good<br />
Int-1<br />
Int-2<br />
Poor<br />
Sur<strong>vie</strong> médiane<br />
80 mois<br />
45 mois<br />
14 mois<br />
4 mois<br />
The new WHO classification-based<br />
Prognostic Scoring System (WPSS)<br />
Overall survival and AML risk<br />
assessments in MDS by WPSS (2)<br />
WHO category<br />
Variable<br />
Karyotype<br />
Transfusion<br />
requirement<br />
RA, RARS,<br />
del(5q)<br />
0<br />
Good<br />
No<br />
0 (Very low)<br />
RCMD,<br />
RCMD-RS<br />
1<br />
Intermediate<br />
Regular<br />
RAEB-<br />
1<br />
2<br />
Poor<br />
–<br />
RAEB-2<br />
3<br />
–<br />
–<br />
Risk group<br />
Very low<br />
Low<br />
Intermediate<br />
High<br />
Very high<br />
Risk group<br />
Very low<br />
Low<br />
Intermediate<br />
High<br />
Very high<br />
WPSS risk<br />
groups<br />
1 (Low)<br />
2 (Intermediate)<br />
3–4 (High)<br />
5–6 (Very high)<br />
Malcovati L, <strong>et</strong> al. J Clin Oncol. 2007;23:3503-10.<br />
Malcovati L, <strong>et</strong> al. J Clin Oncol. 2007;23:3503-10.<br />
6
DIU ONCOGERIATRIE Universités Paris 5 & 6 Année 2008<br />
Anémie <strong>et</strong> suj<strong>et</strong>s âgés<br />
Traitements des faibles risques<br />
TRANSFUSION<br />
CHELATION DU FER<br />
EPO<br />
THALIDOMIDE<br />
REVLIMIDE<br />
ACIDE VALPROIQUE<br />
Myélodysplasie : Classification OMS<br />
5q- syndrome<br />
Myelodysplastic syndrome,<br />
unclassifiable<br />
Refractory anemia<br />
15% 6% (myelodysplastic syndrome) w ith<br />
4%<br />
excess blasts 1<br />
Refractory anemia<br />
18%<br />
29%<br />
(myelodysplastic syndrome) w ith<br />
excess blasts 2<br />
Refractory anemia w ith ringed<br />
sideroblasts<br />
15%<br />
13%<br />
Refractory anemia w ithout ringed<br />
sideroblasts<br />
Faible risque 77%:<br />
Refractory cytopenia<br />
(myelodysplastic syndrome) w ith<br />
multilineage dysplasia<br />
• Anémie lors d’ Insuffisance rénale chronique<br />
Foley Rn J Am Soc Nephrol998;9; Samac Mj Circulation ,2003;108<br />
• Anomalie de la fonction ventriculaire gauche<br />
• Événements cardio vasculaires<br />
• Mortalité<br />
• Anémie chez des suj<strong>et</strong>s âgés sans Insuffisance rénale<br />
Izaks Gj JAMA.1999;281;Chaves Ph J Am Geriatr Soc .2004;52<br />
Penninx Bw J Am Geriatr Soc 004;52 ;Thomas Dr J Gerontol A Biol Sci Med Sci,2004;59<br />
Cull<strong>et</strong>on Bf,Blood2006;107<br />
• Augmentation de la mortalité<br />
• Qualité de <strong>vie</strong> diminuée<br />
• Hospitalisations plus fréquentes<br />
• Augmentation des accidents vasculaires<br />
Transfusions érythrocytaires<br />
Transfusions érythrocytaires<br />
Indications transfusionnelles<br />
‣ Seuil d’Hb<br />
Le seuil critique d’Hb pour des transfusions érythrocytaires se<br />
situe généralement à 8 g/dL<br />
• Toutefois, ce seuil a généralement été fixé pour des<br />
populations plus jeunes, hospitalisées, <strong>et</strong>c…<br />
• seuil supérieur à 8 g/dL dans toutes les circonstances avec<br />
une co-morbidité associée ( consommation d'O2)<br />
‣ Qualité de <strong>vie</strong><br />
La finalité de la transfusion est de participer au maintien optimal<br />
d'un certain degré de qualité de <strong>vie</strong>. Il con<strong>vie</strong>nt d'évaluer l'impact<br />
de la transfusion sur l'asthénie physique aux efforts de la <strong>vie</strong><br />
courante, son r<strong>et</strong>entissement sur les capacités intellectuelles<br />
voire le comportement pour fixer le seuil transfusionnel, qui sera<br />
aussi individualisé que possible<br />
Volume à transfuser<br />
Nb de CGR à apprécier en fonction :<br />
- du volume sanguin total du patient<br />
- de la concentration d’Hb souhaitée (∆ Hb)<br />
En général chez l'adulte : 2 ou 3 CGR, renouvelés dans certains<br />
cas le lendemain afin d'atteindre le seuil souhaité<br />
D’une façon générale, il est donc souhaitable lors de chaque série<br />
de transfuser un nombre suffisant de CGR, de façon à remonter le<br />
taux d’Hb au dessus de 11 g/dL environ, pour éviter que le patient<br />
ait en permanence un syndrome anémique.<br />
Hémochromatose<br />
• Sur<strong>vie</strong>nt dans 30% des patients porteurs de<br />
<strong>SMD</strong><br />
• Apparaît après 20 CG ce qui correspond a<br />
une ferritine de 1000mg<br />
• Entraîne des complications cardiaques en 4<br />
ans<br />
• Une prévention perm<strong>et</strong> d’améliorer la sur<strong>vie</strong><br />
Nécessite une prévention<br />
• Suj<strong>et</strong>s les plus jeunes :<br />
moins de 70 ans (75%)<br />
Hémochromatose<br />
• Sur<strong>vie</strong> supérieure à 4 ans :<br />
• Low; Int -1<br />
• Pas de comorbidité associée<br />
• Greffe Allogénique<br />
7
DIU ONCOGERIATRIE Universités Paris 5 & 6 Année 2008<br />
Guidelines for treatment of iron<br />
overload in patients with MDS<br />
Consensus me<strong>et</strong>ing in Florence (MDS<br />
Foundation)<br />
• Ferritin>1000µg/ml<br />
or 2 units/months for at least 1 year<br />
• No erythroid response to primary therapy or<br />
ineligible for primary therapy<br />
• Survival more than 1 year<br />
• Presence of compromised organ function related<br />
to Iron overload<br />
Hémochromatose<br />
• Mesure de la Surcharge de fer<br />
• Ponction biopsie hépatique difficilement faisable<br />
• IRM hépatique bonne corrélation<br />
• http://oernst.f5lvg.free.fr/liver/iron.html<br />
• Corrélation entre le taux de la ferritine <strong>et</strong> le risque<br />
de complication cardiaque (2500ng/ml)<br />
• Le nombre de concentrés globulaires<br />
Total body iron stores (mg/kg)<br />
300<br />
250<br />
200<br />
150<br />
100<br />
50<br />
CoIHF <strong>et</strong> stock en fer de<br />
l’organisme<br />
0<br />
0 5 10 15 20 25<br />
LIC (mg/g dry weight)<br />
Regression line and 95% confidence limits (upper and lower) are shown<br />
LIC = liver iron content<br />
• Twenty-five patients with<br />
iron overload, cirrhosis,<br />
and liver samples ≥1 mg<br />
dry weight, were<br />
assessed<br />
• The results<br />
demonstrated the linear<br />
relationship b<strong>et</strong>ween<br />
total body iron stores<br />
and LIC levels (r = 0.98,<br />
p
DIU ONCOGERIATRIE Universités Paris 5 & 6 Année 2008<br />
Efficacité<br />
Efficacité<br />
Tolérance<br />
Eff<strong>et</strong>s secondaires<br />
◘ Troubles digestifs - rash cutané<br />
Augmentation créatinine > 33% de la<br />
valeur<br />
◘ Dans 40% des cas<br />
◘ Au delà des valeurs normales dans 16%<br />
(
DIU ONCOGERIATRIE Universités Paris 5 & 6 Année 2008<br />
<strong>SMD</strong> : Epo sérum / Hémoglobine<br />
Patients<br />
Total population n=419<br />
GFM prospective trials<br />
epoi<strong>et</strong>in alfa+ filgrastim<br />
Darbepoi<strong>et</strong>in+/- G-CSF<br />
epoi<strong>et</strong>in b<strong>et</strong>a+ ATRA (EPO arm)<br />
n=133<br />
30<br />
62<br />
41<br />
JACOBS A, BJH, 1989<br />
Patients<br />
Patients<br />
• Inclusion criteria: MDS, WHO classification in 25 GFM<br />
centers<br />
WHO classification<br />
RA<br />
%<br />
14<br />
N<br />
61<br />
• Treatment b<strong>et</strong>ween 1998 and 2006:<br />
– epoi<strong>et</strong>in alpha <strong>et</strong> b<strong>et</strong>a (Eprex, OrthoBiotech/ Neorecormon, Roche)<br />
20000 UI X 3 /week<br />
– darbepoi<strong>et</strong>in alfa (Aranesp, Amgen) 300µg/week<br />
RARS<br />
RAEB-1<br />
RAEB-2<br />
RCMD<br />
19<br />
21<br />
6<br />
16<br />
83<br />
92<br />
26<br />
68<br />
– G-CSF (filgrastim, Amgen; lenograstim, Chugai)<br />
RCMD-RS<br />
13<br />
58<br />
• Evaluation of response to EPO at week 12 with IWG 2000<br />
and IWG 2006 criteria<br />
5q- syndrome<br />
unclassified<br />
4<br />
3<br />
17<br />
14<br />
Patients characteristics<br />
Response<br />
(IWG 2000 and IWG 2006)<br />
EPO level (UI/l, median, range)<br />
>500 (n=, % of patients)<br />
200<br />
na<br />
Transfused (n ,% of patients )<br />
Treatment<br />
EPO alfa<br />
EPO b<strong>et</strong>a<br />
EPO+G-CSF<br />
DAR<br />
DAR+G-CSF<br />
76 (6-5665)<br />
29 (7%)<br />
256 (61%)<br />
94 (22%)<br />
69 (17%)<br />
227 (54%)<br />
53<br />
122<br />
80<br />
126<br />
28<br />
Response<br />
(IWG 2000)<br />
Major<br />
Minor<br />
Minor response=88<br />
(IWG 2000)<br />
262/419<br />
174<br />
88<br />
63%<br />
41%<br />
22%<br />
63% (n=56) = no response<br />
37% (n=32)= response<br />
Response rate (IWG 2006) 49% n=206<br />
IWG 2006<br />
10
DIU ONCOGERIATRIE Universités Paris 5 & 6 Année 2008<br />
Predictive factors of response<br />
in univariate analysis (IWG 2006)<br />
WHO<br />
RA<br />
RCMD<br />
RARS<br />
RCMD-RS<br />
RAEB-1<br />
RAEB-2<br />
5q- syndrome<br />
rate of response (%)<br />
n= 262<br />
62%<br />
62%<br />
47%<br />
48%<br />
46%<br />
23%<br />
52%<br />
ns<br />
ns<br />
Predictive factors of response in<br />
univariate analysis (IWG 2006)<br />
EPO level<br />
EPO200<br />
na<br />
Transfusion<br />
No transfusion<br />
IPSS score<br />
low (38%)<br />
int-1 (41%)<br />
int-2 (9%)<br />
high (1.5%)<br />
na (14.5%)<br />
response rate<br />
total (%)<br />
60% (150/248)<br />
29% (27/92)<br />
41% (26/63)<br />
37% (86/232)<br />
67% (128/191)<br />
61%(88/145)<br />
52% (89/171)<br />
21% (8/38)<br />
0% (0/6)<br />
49% (30/61)<br />
p value<br />
DIU ONCOGERIATRIE Universités Paris 5 & 6 Année 2008<br />
Comparison of PFS and OS<br />
in IMRAW database and GFM<br />
Stratification and matching on FAB (RA, RARS and RAEB)<br />
and IPSS low/int-1 vs int-2/high)<br />
290 patients in the GFM group and 290 patients in the IMRAW database<br />
CONCLUSIONS<br />
• Predictive factors of response to EPO<br />
1. EPO level
DIU ONCOGERIATRIE Universités Paris 5 & 6 Année 2008<br />
Revlimid dans les Low –Int1 non 5q-<br />
Raza A Blood 2008<br />
• Réponse <strong>et</strong> durée<br />
IWG 2000<br />
214 Patients<br />
Moins de 4 culots<br />
Plaqu<strong>et</strong>tes >150 000<br />
Durée courte pour Traitement<br />
LDH
DIU ONCOGERIATRIE Universités Paris 5 & 6 Année 2008<br />
Vidaza dans les Faibles risques<br />
Lyons RM Blood 2007 Abst819<br />
• Teste 3 doses de vidaza<br />
<strong>SMD</strong> (87% de faible<br />
risque)<br />
Hb
DIU ONCOGERIATRIE Universités Paris 5 & 6 Année 2008<br />
Carte des centres<br />
Groupe Français des<br />
Myélodysplasies<br />
Site intern<strong>et</strong> du GFM :<br />
www.gfmgroup.org<br />
Site du registre : www.myelodysplasie.n<strong>et</strong><br />
(l’inscription préalable au GFM est nécessaire pour y accéder)<br />
15