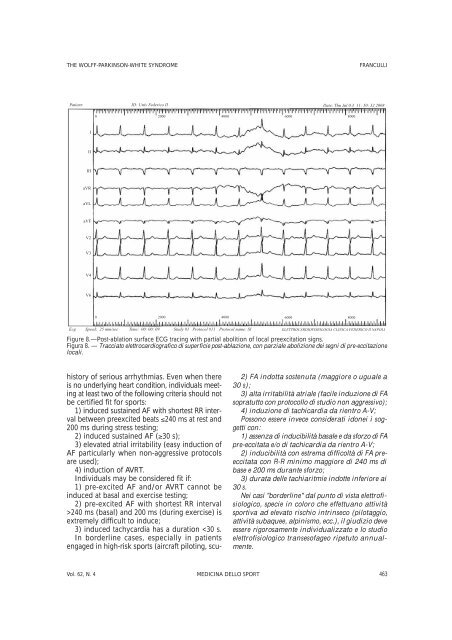
THE WOLFF-PARKINSON-WHITE SYNDROME FRANCULLI Patient: ID: Univ Federico II Date: Thu Jul 0.3 11: 50: 32 2008 I II III aVR aVL aVF V2 V3 V4 V6 0 2000 0 2000 history of serious arrhythmias. Even when there is no underly<strong>in</strong>g heart condition, <strong>in</strong>dividuals meet<strong>in</strong>g at least two of the follow<strong>in</strong>g criteria should not be certified fit for <strong>sport</strong>s: 1) <strong>in</strong>duced susta<strong>in</strong>ed AF with shortest RR <strong>in</strong>terval between preexcited beats ≤240 ms at rest and 200 ms dur<strong>in</strong>g stress test<strong>in</strong>g; 2) <strong>in</strong>duced susta<strong>in</strong>ed AF (≥30 s); 3) elevated atrial irritability (easy <strong>in</strong>duction of AF particularly when <strong>non</strong>-aggressive protocols are used); 4) <strong>in</strong>duction of AVRT. Individuals may be considered fit if: 1) pre-excited AF and/or AVRT cannot be <strong>in</strong>duced at basal and exercise test<strong>in</strong>g; 2) pre-excited AF with shortest RR <strong>in</strong>terval >240 ms (basal) and 200 ms (dur<strong>in</strong>g exercise) is extremely difficult to <strong>in</strong>duce; 3) <strong>in</strong>duced tachycardia has a duration
FRANCULLI THE WOLFF-PARKINSON-WHITE SYNDROME ba div<strong>in</strong>g, alp<strong>in</strong>e <strong>sport</strong>s, etc.), electrophysiological judgement should be made on a case-bycase basis, and transesophageal EPS repeated yearly. Regular EPS with transesophageal pac<strong>in</strong>g (every 3 years) is recommended also <strong>in</strong> young persons and <strong>in</strong> those aged over 30 years due to possible spontaneous alterations <strong>in</strong> electrophysiologic WPW parameters. F<strong>in</strong>ally, <strong>in</strong> our op<strong>in</strong>ion, the difference between competitive and <strong>non</strong>-competitive <strong>sport</strong>s, whether there be medicolegal implications, is irrelevant as regards cardiovascular effort and cardiovascular risk. From an ethical viewpo<strong>in</strong>t it would be correct for both the <strong>sport</strong>s physician and the cardiologist to extend these assessment criteria to <strong>non</strong>competitive <strong>sport</strong>s. We believe this case holds particular <strong>in</strong>terest for several reasons, foremost from the viewpo<strong>in</strong>t of the electrophysiological cardiologist: the anatomic peculiarity of preexcitation with epicardial extension; the family history of WPW, which is sometimes associated with the condition, particularly <strong>in</strong> high-risk <strong>in</strong>dividuals and those with multiple abnormal pathways, <strong>in</strong> a significantly higher percent than <strong>in</strong> the general population; 1-3 and from the viewpo<strong>in</strong>t of the <strong>sport</strong>s physician: the mild symptoms <strong>in</strong> contrast with the elevated risk. We wish to underl<strong>in</strong>e that when assess<strong>in</strong>g persons affected with the WPW syndrome, the <strong>sport</strong>s physician should not be misled by an absence of symptoms which may also occur <strong>in</strong> high-risk persons. In addition, we believe that the assessment criteria should be applied with the same attention to amateur athletes as to those engaged <strong>in</strong> <strong>non</strong> competitive <strong>sport</strong>s, us<strong>in</strong>g at least EPS with transesophageal pac<strong>in</strong>g, especially <strong>in</strong> persons with even mild symptoms. 25 F<strong>in</strong>ally, <strong>in</strong> asymptomatic patients with WPW we stress the diagnostic utility of transesophageal EPS, a useful, <strong>in</strong>expensive method, which is well accepted by patients and can be performed on an out-patient basis, does not <strong>in</strong>volve exposure to radiation, and <strong>in</strong> many types of supraventricular arrhythmias has a diagnostic performance similar to that of endocavitary EPS. 7 In high-risk WPW patients, i.e., those with a documented history of arrhythmic episodes or <strong>in</strong> whom serious arrhythmias can be <strong>in</strong>duced at EPS with transesophageal pac<strong>in</strong>g, the usefulness of endocavitary EPS has been proven. Given the good results obta<strong>in</strong>ed with radio-frequency catheter ablation, with an <strong>in</strong>itial efficacy of at least 95% and a low È raccomandata la valutazione elettrofisiologica transesofagea periodica (ogni 3 anni) anche per i casi idonei, sia nei soggetti <strong>in</strong> età evolutiva, che dopo i 30 anni, per possibilità di modificazione spontanea dei parametri elettrofisiologici del WPW. Inf<strong>in</strong>e, a nostro avviso, la differenza tra pratica <strong>sport</strong>iva agonistica e <strong>non</strong>, se ha una sua ragione di esistere da un punto di vista medico-legale, diventa assolutamente irrilevante <strong>in</strong> relazione all’impegno ed al rischio cardiovascolare. Da un punto di vista etico sarebbe qu<strong>in</strong>di corretto che il Medico dello Sport, così come il Cardiologo, estendessero tali criteri valutativi anche all’attività <strong>sport</strong>iva <strong>non</strong> agonistica. Riteniamo questo caso cl<strong>in</strong>ico di particolare <strong>in</strong>teresse per numerose ragioni, prima fra tutte, dal punto di vista del Cardiologo elettrofisologo, la peculiarità anatomica dell’estr<strong>in</strong>secazione anche epicardica della pre-eccitazione, poi la presenza di familiarità, che talvolta accompagna questa patologia ed <strong>in</strong> particolare i soggetti ad alto rischio e quelli con vie anomale multiple <strong>in</strong> percentuale significativamente più elevata che nella popolazione generale1-3 ed <strong>in</strong>f<strong>in</strong>e, dal punto di vista del Medico dello Sport, la s<strong>in</strong>tomatologia sfumata e subdola <strong>in</strong> contrasto con il rischio elevato. Infatti, ci preme sottol<strong>in</strong>eare come lo Specialista <strong>in</strong> Medic<strong>in</strong>a dello Sport, nella valutazione dei soggetti affetti da s<strong>in</strong>drome di WPW, debba diffidare dell’assenza di s<strong>in</strong>tomatologia che può verificarsi anche nei soggetti a rischio alto, ma anche che, a nostro avviso, i criteri valutativi dovrebbero essere messi <strong>in</strong> essere con la stessa attenzione anche negli atleti amatoriali e nei <strong>non</strong> agonisti, praticando almeno lo studio elettrofisiologico transesofageo, specie <strong>in</strong> soggetti con s<strong>in</strong>tomatologia anche solo sfumata 25. Inf<strong>in</strong>e, nei soggetti as<strong>in</strong>tomatici affetti da s<strong>in</strong>drome di WPW ribadiamo l’utilità diagnostica dello studio elettrofisiologico transesofageo, una metodica utile e a basso costo, bene accettata dai pazienti ed eseguibile ambulatoriamente, che <strong>non</strong> richiede esposizione radiologica a pazienti ed operatori e che, <strong>in</strong> molte aritmie sopraventricolari, ha una performance diagnostica simile <strong>allo</strong> SEF endocavitario 7. Nei soggetti affetti da s<strong>in</strong>drome di WPW ad alto rischio, cioè che abbiano già avuto episodi aritmici documentati o che risult<strong>in</strong>o <strong>in</strong>ducibili per aritmie m<strong>in</strong>acciose <strong>allo</strong> studio transesofageo, è accertata l’utilità dello studio endocavitario; visti i buoni risultati della terapia ablativa, la cui efficacia acuta è pari almeno al 95%, essa nei pazienti s<strong>in</strong>tomatici rappresenta la terapia di prima scelta 26, 27, a fronte di complicanze percentualmente molto 464 MEDICINA DELLO SPORT Dicembre 2009