Paediatrics - Queensland Health - Queensland Government
Paediatrics - Queensland Health - Queensland Government
Paediatrics - Queensland Health - Queensland Government

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Meningitis<br />
Meningitis<br />
Recommend<br />
Consult MO immediately:<br />
- - if a sick looking child has no obvious source of infection, which would explain<br />
their symptoms - the diagnosis is meningitis until proven otherwise<br />
- - if the child has been treated with antibiotics but is still not well (they may have<br />
partly treated meningitis with masking of signs)<br />
-- if the child is unwell with prolonged URTI symptoms<br />
Restrict fluids to 50% of maintenance (10mg / kg) unless there are signs of shock -<br />
MO to discuss as soon as possible with a Paediatrician<br />
Parents or carers may notice early, subtle changes in the child’s conscious state.<br />
Their concerns should not be ignored<br />
Perform hearing test 3 months after discharge from hospital<br />
Background<br />
Mortality is probably 5 - 10% in bacterial meningitis. Most children will make<br />
a full recovery, if appropriately treated. Deafness is the most common long term<br />
complication<br />
Hyponatraemic solutions e.g. 4 % dextrose and one-fifth normal saline or one-quarter<br />
normal saline, have no place in the management of meningitis as they may worsen<br />
hyponatraemia and increase the risk of cerebral oedema [1]<br />
Related topics<br />
Fits / convulsions / seizures<br />
Upper respiratory tract infection -<br />
child<br />
Immunisation program<br />
DRS ABCD resuscitation / the collapsed<br />
patient<br />
O 2 delivery systems<br />
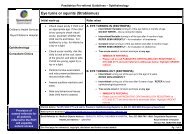
1. May present with<br />
• URTI type symptoms, fever, lethargy, poor feeding<br />
• In young children - non specific signs and symptoms including fever, irritability,<br />
refusing feeds, pallor and a high pitched moaning cry may be present<br />
• In older children - headache, photophobia, neck stiffness [2]<br />
• Leg pain, cold hands and feet<br />
• Abnormal skin colour - pallor or sweating<br />
• Rash in meningococcal disease: usually non blanching petechiae (fine dark red<br />
spots) but may be purpura (like bruises), or less commonly, a ‘flea bitten’ pink / red<br />
maculopapular rash. The rash often develops rapidly, however meningococcal<br />
disease can occur without a rash<br />
• Muscle / joint pains, vomiting, diarrhoea<br />
• Confusion, drowsiness, loss of consciousness<br />
• Bulging fontanelle, fitting<br />
2. Immediate management<br />
• Consult MO immediately<br />
• If altered level of consciousness See DRS ABCD resuscitation / the collapsed<br />
patient<br />
• If fitting see Fits / convulsions / seizures<br />
• Give O 2 to maintain O 2 saturation >95%. If >95% not maintained consult MO.<br />
See O 2 delivery systems<br />
• Insert IV / IO cannula and take FBC, U/E, blood cultures, PCR for Neisseria<br />
meningitis (meningococcal bacteria)<br />
Primary Clinical Care Manual 2011 Controlled copy V 1.0 559