Paediatrics - Queensland Health - Queensland Government
Paediatrics - Queensland Health - Queensland Government
Paediatrics - Queensland Health - Queensland Government

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Ear problems<br />
586<br />
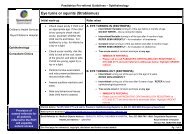
Otitis media with effusion (OME)<br />
Painless non discharging ears, glue ear<br />
Recommend<br />
Review children with bilateral OME at 3 monthly intervals and refer if required<br />
<strong>Health</strong> clinics have targeted hearing health programs to focus on day care and<br />
pre school children where intervention may prevent ear damage and hearing loss.<br />
Personal hygiene in children - washing hands and face and keeping face clear of<br />
nasal discharge is most effective<br />
Provide full immunisation<br />
Background<br />
OME is diagnosed if thick fluid persists in the middle ear usually after AOM<br />
OME results in thick glue like material filling the middle ear which may take many<br />
months to resolve. It is important because children with OME will have impaired<br />
hearing. If hearing is impaired for a significant length of time especially at the critical<br />
age of language learning in the first 5 years it may result in significant long term<br />
disability<br />
Decongestants and antihistamines are not recommended [7]<br />
Steroids are not recommended [1] but inhaled steroids may be trialed in children<br />
where significant nasal obstruction, sneezing etc. suggests allergic rhinitis<br />
Related topics<br />
Acute otitis media<br />
Immunisation program<br />
Controlled copy V1.0<br />
Assessment of the ear<br />
1. May present with<br />
• Usually is asymptomatic<br />
• Parents may be concerned about the child’s hearing<br />
• Diagnosis may also be suspected at routine ear examination, in a child being<br />
followed up after AOM, or in a child referred for medical assessment because of<br />
hearing impairment on testing<br />
• Child may have:<br />
-- past history of recurrent otitis media<br />
-- concerns about speech or language development<br />
• Reported decrease in hearing<br />
• Reported poor hearing leading to learning difficulties<br />
2. Immediate management Not applicable<br />
3. Clinical assessment<br />
• Obtain a complete patient history. See Assessment of the ear<br />
• Perform standard clinical observations<br />
• Perform physical examination. See Assessment of the ear<br />
-- the following may be noted on examination<br />
○ air / fluid level, bubbles behind the ear drum<br />
○ retraction of ear drum<br />
○ limited or absent movement of the ear drum with pneumatic otoscopy.<br />
This is the best way to diagnose - refer to audiology / MO to perform.<br />
Diagnosis is confirmed by tympanometry which shows a type B (stiff ear<br />
drum) pattern<br />
Primary Clinical Care Manual 2011