Paediatrics - Queensland Health - Queensland Government
Paediatrics - Queensland Health - Queensland Government
Paediatrics - Queensland Health - Queensland Government

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
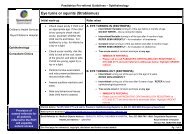
Meningitis<br />
• In the critically ill, shocked or septic child with suspected meningitis e.g.<br />
unresponsive, poorly perfused, purpuric rash, it is appropriate to first give a bolus<br />
of intravenous or intraosseous fluids (initially 10 - 20 mL / kg of normal saline [1])<br />
before giving antibiotics. Otherwise restrict total fluids to 10 mL / kg.<br />
• MO to consult as soon as possible with Paediatrician<br />
3. Clinical assessment<br />
• Obtain as complete a patient history as possible according to the circumstances<br />
of the presentation. Of particular importance in a sick looking child is:<br />
-- -headache, irritability, fever, ask about any rash, neck stiffness<br />
• Perform standard clinical observations +<br />
-- weight (if able)<br />
-- GCS<br />
-- O saturation<br />
2<br />
• Perform physical examination:<br />
-- inspect all skin surfaces for any skin rash especially at pressure points and<br />
under nappies and clothing. Note: petechiae and purpura do not fade on<br />
pressure<br />
-- assess hydration status<br />
-- -inspect and palpate the ears, nose and throat<br />
-- palpate the fontanelle in young baby - feeling for fullness<br />
-- check for neck stiffness - with patient lying down, put hand behind head and<br />
gently raise<br />
-- auscultate the chest for air entry and any added sounds (crackles or wheezes)<br />
• Check vaccination status, especially Hib / meningococcal / conjugate<br />
pneumococcal<br />
4. Management<br />
• Consult MO who will arrange / order:<br />
-- evacuation / hospitalisation<br />
-- monitor clinical observations closely<br />
-- continue IV / IO fluids at 50% of maintenance fluids (10 mL / kg). If the child is<br />
drinking ensure total fluids do not exceed 10 mL / kg (or 50 % of maintenance<br />
fluids)<br />
-- if meningitis is suspected, stat dose of parenteral antibiotics must be given<br />
before transfer to hospital. Blood samples for culture and PCR should be<br />
taken where possible but should not delay initial treatment<br />
-- give IV ceftriaxone (can be given by IM route if unable to obtain IV access)<br />
100 mg / kg / dose to a total of 4 grams daily (or 50 mg / kg / dose bd to a total<br />
of 2 grams bd) [3]<br />
• Give paracetamol for fever, pain or distress<br />
See Simple analgesia back cover<br />
5. Follow up<br />
All children with suspected meningitis should be managed in an appropriately<br />
equipped hospital<br />
Notify the Public <strong>Health</strong> Unit of any suspected case of bacterial meningitis as<br />
soon as possible<br />
Chemoprophylaxis will be required for close contacts of a patient with either<br />
meningococcal or Hib meningitis. Unvaccinated contacts of Hib meningitis