

sign130
sign130
sign130

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
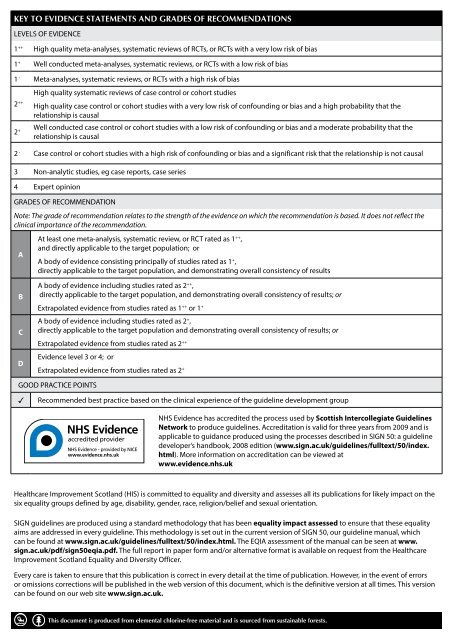
KEY TO EVIDENCE STATEMENTS AND GRADES OF RECOMMENDATIONS<br />
LEVELS OF EVIDENCE<br />
1 ++ High quality meta-analyses, systematic reviews of RCTs, or RCTs with a very low risk of bias<br />
1 + Well conducted meta-analyses, systematic reviews, or RCTs with a low risk of bias<br />
1 - Meta-analyses, systematic reviews, or RCTs with a high risk of bias<br />
2 ++<br />
High quality systematic reviews of case control or cohort studies<br />
High quality case control or cohort studies with a very low risk of confounding or bias and a high probability that the<br />
relationship is causal<br />
2 + Well conducted case control or cohort studies with a low risk of confounding or bias and a moderate probability that the<br />
relationship is causal<br />
2 - Case control or cohort studies with a high risk of confounding or bias and a significant risk that the relationship is not causal<br />
3 Non-analytic studies, eg case reports, case series<br />
4 Expert opinion<br />
GRADES OF RECOMMENDATION<br />
Note: The grade of recommendation relates to the strength of the evidence on which the recommendation is based. It does not reflect the<br />
clinical importance of the recommendation.<br />
A<br />
B<br />
C<br />
D<br />
At least one meta-analysis, systematic review, or RCT rated as 1 ++ ,<br />
and directly applicable to the target population; or<br />
A body of evidence consisting principally of studies rated as 1 + ,<br />
directly applicable to the target population, and demonstrating overall consistency of results<br />
A body of evidence including studies rated as 2 ++ ,<br />
directly applicable to the target population, and demonstrating overall consistency of results; or<br />
Extrapolated evidence from studies rated as 1 ++ or 1 +<br />
A body of evidence including studies rated as 2 + ,<br />
directly applicable to the target population and demonstrating overall consistency of results; or<br />
Extrapolated evidence from studies rated as 2 ++<br />
Evidence level 3 or 4; or<br />
Extrapolated evidence from studies rated as 2 +<br />
GOOD PRACTICE POINTS<br />
Recommended best practice based on the clinical experience of the guideline development group<br />
NHS Evidence has accredited the process used by Scottish Intercollegiate Guidelines<br />
Network to produce guidelines. Accreditation is valid for three years from 2009 and is<br />
applicable to guidance produced using the processes described in SIGN 50: a guideline<br />
developer’s handbook, 2008 edition (www.sign.ac.uk/guidelines/fulltext/50/index.<br />
html). More information on accreditation can be viewed at<br />
www.evidence.nhs.uk<br />
Healthcare Improvement Scotland (HIS) is committed to equality and diversity and assesses all its publications for likely impact on the<br />
six equality groups defined by age, disability, gender, race, religion/belief and sexual orientation.<br />
SIGN guidelines are produced using a standard methodology that has been equality impact assessed to ensure that these equality<br />
aims are addressed in every guideline. This methodology is set out in the current version of SIGN 50, our guideline manual, which<br />
can be found at www.sign.ac.uk/guidelines/fulltext/50/index.html. The EQIA assessment of the manual can be seen at www.<br />
sign.ac.uk/pdf/sign50eqia.pdf. The full report in paper form and/or alternative format is available on request from the Healthcare<br />
Improvement Scotland Equality and Diversity Officer.<br />
Every care is taken to ensure that this publication is correct in every detail at the time of publication. However, in the event of errors<br />
or omissions corrections will be published in the web version of this document, which is the definitive version at all times. This version<br />
can be found on our web site www.sign.ac.uk.<br />
This document is produced from elemental chlorine-free material and is sourced from sustainable forests.