Netherton syndrome: Successful use of topical tacrolimus ... - Colleges
Netherton syndrome: Successful use of topical tacrolimus ... - Colleges
Netherton syndrome: Successful use of topical tacrolimus ... - Colleges

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
290<br />
Blackwell Oxford, IJD International 1365-4632 Blackwell 45 UK Publishing Journal Ltd Ltd, <strong>of</strong> Dermatology 2006<br />
Case report<br />
Calcineurin Saif CASE and REPORT Al-Khenaizan inhibitors in <strong>Netherton</strong> <strong>syndrome</strong><br />
<strong>Netherton</strong> <strong>syndrome</strong>: <strong>Successful</strong> <strong>use</strong> <strong>of</strong> <strong>topical</strong> <strong>tacrolimus</strong> and<br />
pimecrolimus in four siblings<br />
Ghada Bin Saif,<br />
From the Division <strong>of</strong> Dermatology,<br />
Department <strong>of</strong> Medicine, King Fahad National<br />
Guard Hospital, King Abdulaziz Medical<br />
City-Riyadh, Saudi Arabia<br />
Correspondence<br />
Sultan Al-Khenaizan, MBBS,<br />
FRCPC,<br />
DABD<br />
Division <strong>of</strong> Dermatology, Department <strong>of</strong><br />
Medicine<br />
King Fahad National Guard Hospital<br />
PO Box 22490<br />
Riyadh 11426<br />
Kingdom <strong>of</strong> Saudi Arabia<br />
E-mail: khenaizans@ngha.med.sa<br />
Introduction<br />
MBBS,<br />
and Sultan Al-Khenaizan, MBBS, FRCPC, DABD<br />
<strong>Netherton</strong>’s <strong>syndrome</strong> (NS) is a rare autosomal recessive disease<br />
comprised <strong>of</strong> ichthyosis in the form <strong>of</strong> ichthyosis linearis<br />
circumflexa (ILC), hair shaft defects including trichorrhexis<br />
invaginata, trichorrhexis nodosa and pili torti and atopic<br />
1,2<br />
manifestations with an elevated IgE level. Tacrolimus and<br />
3<br />
pimecrolimus belong to the family <strong>of</strong> calcineurin inhibitors.<br />
They bind cytoplasmic proteins and the resulting complex<br />
binds calcineurin, inhibiting its ability to dephosphorylate the<br />
nuclear factor <strong>of</strong> activated T cells (NF-AT), thus suppressing<br />
3<br />
gene transcription. There have been conflicting reports <strong>of</strong> the<br />
<strong>use</strong>fulness <strong>of</strong> <strong>tacrolimus</strong> in NS patients, with systemic absorp-<br />
4–6<br />
tion being the main adverse outcome. We report four Saudi<br />
siblings (two boys and two girls) with NS who were treated<br />
with <strong>topical</strong> <strong>tacrolimus</strong> and pimecrolimus with good control<br />
<strong>of</strong> their skin disease without any toxic effect.<br />
Case Report<br />
Patient A was a 12-year-old Saudi girl who presented with<br />
generalized scaly skin eruption since birth. The eruption waxes<br />
and wanes, but never completely clears. The patient <strong>use</strong>d<br />
mometasone furoate 0.1% (Elocom, Schering, Belgium)<br />
ointments extensively for many years without medical supervision,<br />
which temporarily helps the eruption. The parents were<br />
first-degree cousins. The skin disease and other social reasons led<br />
the child to quit school few years ago. Physical examination<br />
revealed small-for-age growth parameters. Facial examination<br />
Abstract<br />
<strong>Netherton</strong>’s <strong>syndrome</strong> (NS) is a rare autosomal recessive disease comprised <strong>of</strong> ichthyosis in<br />
the form <strong>of</strong> ichthyosis linearis circumflexa, hair shaft defects and atopic manifestations with an<br />
elevated IgE level. Various therapeutic options have been <strong>use</strong>d in NS with variable success.<br />
Tacrolimus and pimecrolimus belong to the family <strong>of</strong> calcineurin inhibitors. They bind<br />
cytoplasmic proteins and the resulting complex binds calcineurin, inhibiting its ability to<br />
dephosphorylate the nuclear factor <strong>of</strong> activated T cells, thus suppressing gene transcription.<br />
There have been conflicting reports <strong>of</strong> the <strong>use</strong>fulness <strong>of</strong> <strong>tacrolimus</strong> in NS patients, with systemic<br />
absorption being the main adverse outcome. Here we report four Saudi siblings (two boys and<br />
two girls) with NS who were treated with <strong>topical</strong> <strong>tacrolimus</strong> and pimecrolimus with good control<br />
<strong>of</strong> their skin disease without any toxic effect. To our knowledge, this is the second report <strong>of</strong> the<br />
<strong>use</strong> <strong>of</strong> <strong>topical</strong> pimecrolimus in NS in the English literature.<br />
revealed small eyes, narrow palpebral fissure and frontal<br />
bossing. Skin examination revealed generalized, polycyclic scaly<br />
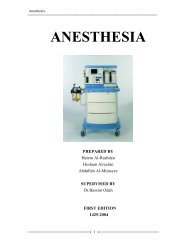
erythematous plaques with doubled-edged scaling (Fig. 1).<br />
These were compatible with the clinical diagnosis <strong>of</strong> ichthyosis<br />
linearis circumflexa (ILC). Scalp examination revealed diff<strong>use</strong><br />
scaling with short brittle hair. There was loss <strong>of</strong> hair over the<br />
outer third <strong>of</strong> both eyebrows. The patient’s teeth, nails, eyes and<br />
mucous membrane were normal. Blood investigation revealed:<br />
3<br />
eosinophilia with absolute eosinophil count <strong>of</strong> 1.5 × 10 cell<br />
3<br />
3<br />
3<br />
per mm (normal < 0.7 × 10 cell per mm ), high IgE level <strong>of</strong><br />
5923.4 IU/mL (Normal < 400 IU/mL). Morning serum cortisol<br />
level was low at 23 nmol/L (normal: 119–618 nmol/L). Adrenal<br />
suppression was confirmed by a blunted response to a short<br />
Synacthen stimulation test. This recovered spontaneously<br />
after 1 year.<br />
Patients B, C and D were a 6-year-old boy, 3-year-old girl and<br />
40-day-old, respectively; siblings <strong>of</strong> patient A. They presented<br />
with generalized scaly skin eruption since birth. Physical<br />
examination revealed small-for-age growth parameters. Facial<br />
examination revealed rosy telangiectatic cheeks, small eyes,<br />
narrow palpebral fissures, large ears, pinched nose, frontal<br />
bossing and prominent occiput. Skin examination <strong>of</strong> patients<br />
B and C revealed generalized, polycyclic scaly erythematous<br />
plaques with doubled-edged scaling at the margins. These were<br />
compatible with the clinical diagnosis <strong>of</strong> ILC. Their scalp<br />
examination showed diff<strong>use</strong> scaling with short brittle hair.<br />
They had loss <strong>of</strong> hair over the outer third <strong>of</strong> both eyebrows.<br />
Patient D’s skin examination revealed generalized erythroderma<br />
with extensive scalp scaling. The patient’s nails, eyes<br />
International Journal <strong>of</strong> Dermatology 2007, 46,<br />
290–294 © 2006 The International Society <strong>of</strong> Dermatology
Saif and Al-Khenaizan<br />
Figure 1 Left leg <strong>of</strong> patient A showing multiple polycyclic red<br />
plaques with double-edged scales constituting ichthyosis linearis<br />
circumflexa<br />
and mucous membranes were normal. None <strong>of</strong> these patients<br />
had temperature instability, hypernatraemic dehydration nor<br />
documented secondary skin infection. Blood investigation<br />
revealed: oesinophilia with absolute oesinophil counts were<br />
3<br />
3<br />
3<br />
2.7 × 10 and 1.9 × 10 cell per mm for patients B and C, respec-<br />
3<br />
3<br />
tively (normal < 0.7 × 10 cell per mm ). IgE levels were 2202<br />
and 1522.5 IU/mL for patients B and C, respectively (normal<br />
< 400 IU/mL). Histological examination <strong>of</strong> lesional skin biopsies<br />
from the trunk <strong>of</strong> patients A, B, and C revealed parakeratotic<br />
hyperkeratosis and spongiosis compatible with ILC. Trichorrhexis<br />
invaginata was observed in light microscopy <strong>of</strong> scalp<br />
hair obtained from all three patients (Fig. 2). Other hair findings<br />
were trichorrhexis nodosa and pili torti. Based on these findings,<br />
<strong>Netherton</strong>’s <strong>syndrome</strong> was diagnosed.<br />
Patient A was treated with <strong>topical</strong> <strong>tacrolimus</strong> ointment<br />
0.03%, which was compounded in our hospital pharmacy<br />
by mixing the content <strong>of</strong> <strong>tacrolimus</strong> (Progaf, Fujisawa, UK)<br />
capsules into petroleum jelly, and was applied twice a day on<br />
red areas with marked improvement. As the <strong>tacrolimus</strong> blood<br />
level carried out 2 weeks later was undetectable, the <strong>tacrolimus</strong><br />
concentration was increased to 0.1%, which induced<br />
even better improvement with marked reduction in erythema<br />
and scaling. The patient was switched to Protopic oinment<br />
0.1% once it became available in our hospital.<br />
Similarly, patients B and C were treated with <strong>topical</strong><br />
<strong>tacrolimus</strong> 0.03% (Protopic, Fujisawa) ointment twice a day<br />
for 2 years, with no adverse effects noted. Once it became<br />
available in our hospital, and after 2 years <strong>of</strong> <strong>tacrolimus</strong> <strong>use</strong>,<br />
all three patients were switched to pimecrolimus 1% (Elidel,<br />
Novartis, Switzerland) cream twice a day with a comparable<br />
control <strong>of</strong> their skin disease. Patient D was initially treated<br />
with alclometasone dipropionate 0.05% (Perderm, Schering,<br />
Belgium) ointment twice a day with reasonable control <strong>of</strong> the<br />
Calcineurin inhibitors in <strong>Netherton</strong> <strong>syndrome</strong><br />
Case report<br />
Figure 2 Light microscopy <strong>of</strong> scalp hair from patient A showing<br />
trichorrhexis invaginata<br />
skin eruption. At 5 months <strong>of</strong> age the patient was started on<br />
pimecrolimus 1% (Elidel, Novartis) cream twice a day with<br />
good improvement. In all four patients, the two medications<br />
were <strong>use</strong>d intermittently with application on the first appearance<br />
<strong>of</strong> redness and discontinuation upon clearance. All four<br />
patients demonstrated marked reduction to nearly complete<br />
clearance <strong>of</strong> erythema, scaling and pruritus. The disease still<br />
waxes and wanes, requiring short intermittent courses <strong>of</strong><br />
fluticasone propionate ointment 0.005% (Cutivate, Glaxo<br />
KlineSmith, UK) for few days. Trichorrhexis invaginata<br />
and hair fragility did not improve. There was no patient or<br />
parental report <strong>of</strong> burning sensation or any other local or<br />
systemic adverse effects and no cutaneous infections were<br />
observed. We noticed no significant difference in the level<br />
<strong>of</strong> control <strong>of</strong> the skin eruption between <strong>topical</strong> <strong>tacrolimus</strong><br />
and pimecrolimus. We could not compare the response to<br />
calcineurin inhibitors and the response to Elocom beca<strong>use</strong><br />
the latter was <strong>use</strong>d before presentation and was stopped by the<br />
authors immediately. The parents, however, stated that the<br />
response to <strong>tacrolimus</strong> and pimcrolimus was comparable to<br />
steroids. Tacrolimus blood levels were checked initially periodically<br />
every 3–4 months and were mostly undetectable.<br />
Occasionally, it was just detectable, ranging from 1.6 ng/mL<br />
to 2.7 ng/mL, and significantly below the therapeutic range<br />
for transplants patients (5–10 ng/mL). Pimecrolimus blood level<br />
was not performed beca<strong>use</strong> it is not available in our hospital.<br />
Discussion<br />
<strong>Netherton</strong>’s <strong>syndrome</strong> was originally described by <strong>Netherton</strong><br />
1<br />
in 1958. It is a rare disorder comprising ichthyosiform<br />
dermatitis usually in the form <strong>of</strong> ILC, trichorrhexis invaginata<br />
1<br />
and atopic diathesis. The degree <strong>of</strong> skin involvement is vari-<br />
2<br />
able. Newborns with NS may have generalized erythroderma<br />
© 2006 The International Society <strong>of</strong> Dermatology International Journal <strong>of</strong> Dermatology 2007, 46,<br />
290–294<br />
291
292 Case report<br />
Calcineurin inhibitors in <strong>Netherton</strong> <strong>syndrome</strong><br />
2<br />
or a collodion baby phenotype with failure to thrive. Beyond<br />
infancy, skin changes evolve into ILC, which are polycyclic<br />
2<br />
migratory plaques with characteristic double-edged scales.<br />
The finding <strong>of</strong> trichorrhexis invaginata is pathognomic for<br />
7<br />
NS. Other hair shaft findings in NS include pili torti and<br />
8<br />
trichorrhexis nodosa. Atopy may manifest as atopic dermatitis<br />
2<br />
or asthma with marked elevation <strong>of</strong> IgE. Other inconsistent<br />
features include aminoaciduria, mild developmental delay,<br />
2<br />
and impaired cellular immunity. <strong>Netherton</strong>’s <strong>syndrome</strong> may<br />
also be complicated by temperature instability, hypernatremic<br />
8<br />
dehydration and frequent skin infection.<br />
There have been many reports <strong>of</strong> NS in siblings <strong>of</strong> different<br />
9–21<br />
sexes, mostly from consanguineous marriages, suggesting<br />
9,10<br />
autosomal recessive inheritance. The gene defect has been<br />
recently mapped to chromosome 5q 32, and identified as a<br />
mutation in the SPINK5 gene, encoding a serine protease<br />
inhibitor known as lymphoepithelial kasal type related<br />
22–27<br />
inhibitor (LEKTI). This leads to LEKTI deficiency in the<br />
28<br />
epidermis and in hair roots at the protein level. Surprisingly,<br />
Rhagunath et al.<br />
found aberrant expression <strong>of</strong> other proteins,<br />
especially transglutaminases 1 and 3, which may also account<br />
28<br />
for the impaired epidermal barrier in NS.<br />
On reviewing photographs <strong>of</strong> NS patients previously<br />
reported in the literature, we noticed that most patients with<br />
NS have distinct dysmorphic faces. The salient features are<br />
small eyes, frontal bossing, narrow palpebral fissures and a<br />
pinched nose. We believe that this dysmorphic face is not<br />
emphasized in the literature.<br />
Various therapeutic options have been <strong>use</strong>d in NS with<br />
variable success.<br />
Topical steroids are moderately effective, but<br />
the risk <strong>of</strong> systemic absorption, producing Cushing <strong>syndrome</strong>,<br />
29,30<br />
limits their <strong>use</strong>. Systemic and <strong>topical</strong> retinoids <strong>use</strong> is limited<br />
9,16,31,32<br />
by the risk <strong>of</strong> skin lesion aggravation. Other options<br />
have included <strong>topical</strong> calcipotriol, PUVA, cyclosporine and<br />
14,33–37<br />
ammonium lactate 12% lotion (Lac-Hydrin).<br />
Pimecrolimus and <strong>tacrolimus</strong> belong to the family <strong>of</strong><br />
3<br />
calcineurin inhibitors. These macrolactam immunomodulators<br />
exert their effect by binding to cytoplasmic proteins and the<br />
resulting complex binds calcineurin, inhibiting its ability to<br />
3<br />
dephosphorylate NF-AT. NF-AT is a nuclear transcription<br />
factor that facilitates the transcription <strong>of</strong> several growth factor<br />
and inflammatory genes; however, it must be dephosphoryl-<br />
38,39<br />
ated to translocate into the nucleus. These medications<br />
inhibit T-cell proliferation and the production and release<br />
<strong>of</strong> several growth factors and pro-inflammatory cytokines,<br />
including interleukin-2 (IL-2), IL-4, interferonγ(IFNγ) and<br />
3,39<br />
tumor necrosis factorγ(TNFγ). Moreover, they prevent<br />
mast cell release <strong>of</strong> pro-inflammatory mediators including<br />
39–41<br />
histamine, cytokines, tryptase and eicosanoids. Pimecrolimus<br />
shows a selective action on T cells and mast cells as<br />
3,39<br />
opposed to the more pleiotropic targets <strong>of</strong> <strong>tacrolimus</strong>. In<br />
contrast to <strong>tacrolimus</strong>, pimecrolimus does not affect the<br />
differentiation, maturation and functions <strong>of</strong> dendritic cells and<br />
Saif and Al-Khenaizan<br />
42–44<br />
does not induce apoptosis <strong>of</strong> epidermal Langerhans’ cells.<br />
In contrast to corticosteroids, they do not affect endothelial<br />
cells and fibroblasts and therefore do not induce telangiectasia<br />
45<br />
and skin atrophy. The propensity <strong>of</strong> pimecrolimus to pass<br />
through the skin is approximately 90-fold lower than corti-<br />
46<br />
costeroids and approximately ninefold lower than <strong>tacrolimus</strong>.<br />
The differences related to skin permeation may be explained<br />
by the distinct lipophilicity/hydrophilicity distribution within<br />
3<br />
the molecules. The intrinsic capability <strong>of</strong> pimecrolimus and<br />
<strong>tacrolimus</strong> to cross the stratum corneum is similar, whereas<br />
3<br />
further penetration is impaired in the case <strong>of</strong> pimecrolimus.<br />
Tacrolimus and pimecrolimus have been approved by many<br />
3,39<br />
agencies for atopic dermatitis. There have been several<br />
reports <strong>of</strong> the efficacy <strong>of</strong> <strong>tacrolimus</strong> and pimecrolimus in a<br />
variety <strong>of</strong> other inflammatory dermatoses including psoriasis,<br />
4–6,29,47,48<br />
lamellar ichthyosis and NS. Beca<strong>use</strong> patients with NS<br />
may be particularly vulnerable to increased percutaneous<br />
absorption owing to a defective epidermal barrier, it is recom-<br />
5,6,49<br />
mended to monitor the blood drug level closely. Although<br />
systemic absorption <strong>of</strong> <strong>topical</strong> <strong>tacrolimus</strong> in NS has been<br />
reported, some patients may tolerate it without this occurrence,<br />
6<br />
as observed by ourselves and other authors. When switched<br />
to <strong>topical</strong> pimecrolimus, all four <strong>of</strong> our patients maintained a<br />
comparable control <strong>of</strong> their skin disease. The lesser epidermal<br />
permeation <strong>of</strong> pimecrolimus in comparison with <strong>tacrolimus</strong><br />
may <strong>of</strong>fer an added advantage in patients with NS. This,<br />
however, has to be confirmed by blood drug level studies in<br />
patients with NS. Recently, Oji et al.<br />
reported a 10-year-old<br />
boy with NS who was initially treated successfully with<br />
<strong>topical</strong> <strong>tacrolimus</strong> 0.03% ointment, which was discontinued<br />
50<br />
beca<strong>use</strong> <strong>of</strong> an increase in the blood drug level to 2.5 ng/mL.<br />
Later, this patient was switched to <strong>topical</strong> pimecrolimus 1%<br />
50<br />
cream with 75% reduction in the skin eruption. Interestingly,<br />
no systemic adverse effects were observed and the blood<br />
50<br />
pimecrolimus level remained low at < 2.4 ng/mL.<br />
The experience reported here on the <strong>use</strong> <strong>of</strong> <strong>topical</strong> <strong>tacrolimus</strong><br />
and pimecrolimus in NS along with previous reports suggest that<br />
this mode <strong>of</strong> treatment is effective, and mostly well-tolerated.<br />
However, caution is needed when using <strong>tacrolimus</strong> and close<br />
monitoring through repeated blood drug levels is warranted<br />
to assure that no significant absorption has occurred.<br />
References<br />
1 <strong>Netherton</strong> EW. A unique case <strong>of</strong> trichorrhexis<br />
nodosa; bamboo hairs. Arch Dermatol 1958;<br />
78:<br />
483–487.<br />
2 DiGiovanna JJ. Ichthyosiform dermatoses: So many<br />
discoveries, so little progress. J Am Acad Dermatol 2004;<br />
51:<br />
S31–S34.<br />
3 Gisondi P, Ellis CN, Girolomoni G. Pimecrolimus in<br />
dermatology: atopic dermatitis and beyond. Int J Clin Pract<br />
2005; 59:<br />
969–974.<br />
4 Allen DM, Esterly NB. Significant systemic absorption <strong>of</strong><br />
International Journal <strong>of</strong> Dermatology 2007, 46,<br />
290–294 © 2006 The International Society <strong>of</strong> Dermatology
Saif and Al-Khenaizan<br />
<strong>tacrolimus</strong> after <strong>topical</strong> application in a patient with lamellar<br />
ichthyosis. Arch Dermatol 2002; 138:<br />
1259–1260.<br />
5 Allen A, Siegfried E, Silverman R, et al. Significant<br />
absorption <strong>of</strong> <strong>topical</strong> <strong>tacrolimus</strong> in 3 patients with<br />
<strong>Netherton</strong> <strong>syndrome</strong>. Arch Dermatol 2001; 137:<br />
747–750.<br />
6 Bens G, Boralevi F, Buzenet C, et al. Topical treatment <strong>of</strong><br />
<strong>Netherton</strong>’s Syndrome with <strong>tacrolimus</strong> ointment without<br />
significant systemic absorption. Br J Dermatol 2003;<br />
149:<br />
224–226.<br />
7 Sybert VP. Disorders <strong>of</strong> the epidermis. In: Sybert VP, ed.<br />
Genetic Skin Disorders.<br />
New York, Oxford: Oxford<br />
University Press, 1997: 5–128.<br />
8 Greene SL, Muller SA. <strong>Netherton</strong>’s <strong>syndrome</strong>. Report <strong>of</strong> a<br />
case and review <strong>of</strong> the literature. J Am Acad Dermatol 1985;<br />
13:<br />
329–337.<br />
9 Caputo R, Vanotti P, Bertani E. <strong>Netherton</strong>’s <strong>syndrome</strong> in<br />
two adult brothers. Arch Dermatol 1984; 120:<br />
220–222.<br />
10 Brodin MB, Porter PS. <strong>Netherton</strong>’s <strong>syndrome</strong>. Cutis 1980;<br />
26:<br />
185–188, 191.<br />
11 Kassis V, Nielsen JM, Klem-Thomsen H, et al. Familial<br />
<strong>Netherton</strong>’s disease. Cutis 1986; 38:<br />
175–178.<br />
12 Stankler L, Cochrane T. <strong>Netherton</strong>’s disease in two sisters.<br />
Br J Dermatol 1967; 79:<br />
187–196.<br />
13 Plantin P, Delaire P, Guillet MH, et al. <strong>Netherton</strong>’s<br />
<strong>syndrome</strong>. Current aspects. Apropos <strong>of</strong> 9 cases. Ann<br />
Dermatol Venereol 1991; 118:<br />
525–530.<br />
14 Wehr RF, Hickman J, Krochmal L. Effective treatment <strong>of</strong><br />
<strong>Netherton</strong>’s <strong>syndrome</strong> with 12% lactate lotion. J Am Acad<br />
Dermatol 1988; 19:<br />
140–142.<br />
15 Hausser I, Anton-Lamprecht I. Severe congenital generalized<br />
exfoliative erythroderma in newborns and infants: a possible<br />
sign <strong>of</strong> <strong>Netherton</strong> <strong>syndrome</strong>. Pediatr Dermatol 1996; 13:<br />
183–199.<br />
16 Judge MR, Morgan G, Harper JI. A clinical and<br />
immunological study <strong>of</strong> <strong>Netherton</strong>’s <strong>syndrome</strong>. Br J<br />
Dermatol 1994; 131:<br />
615–621.<br />
17 Curth HO. <strong>Netherton</strong>’s <strong>syndrome</strong> and ichthyosis linearis<br />
circumflexa. Arch Dermatol 1970; 101:<br />
485.<br />
18 Jones SK, Thomason LM, Surbrugg SK, et al. Neonatal<br />
hypernatraemia in two siblings with <strong>Netherton</strong>’s <strong>syndrome</strong>.<br />
Br J Dermatol 1986; 114:<br />
741–743.<br />
19 Salamon T, Lazovic O, Stenek S. The <strong>Netherton</strong> Syndrome.<br />
Hautarzt 1972; 23:<br />
66–71.<br />
20 Stryk S, Siegfried EC, Knutsen AP. Selective antibody<br />
deficiency to bacterial polysaccharide antigens in patients<br />
with <strong>Netherton</strong> <strong>syndrome</strong>. Pediatr Dermatol 1999; 16:<br />
19–<br />
22.<br />
21 Ansai S, Mitsuhashi Y, Sasaki K. <strong>Netherton</strong>’s <strong>syndrome</strong> in<br />
siblings. Br J Dermatol 1999; 141:<br />
1097–1100.<br />
22 Chavanas S, Garner C, Bodemer C, et al. Localization <strong>of</strong> the<br />
<strong>Netherton</strong> <strong>syndrome</strong> gene to chromosome 5q32, by linkage<br />
analysis and homozygosity mapping. Am J Hum Genet<br />
2000; 66:<br />
914–921.<br />
23 Chavanas S, Bodemer C, Rochat A, et al. Mutations in<br />
SPINK5, encoding a serine protease inhibitor, ca<strong>use</strong><br />
<strong>Netherton</strong> <strong>syndrome</strong>. Nat Genet 2000; 25: 141–142.<br />
Calcineurin inhibitors in <strong>Netherton</strong> <strong>syndrome</strong><br />
Case report<br />
24 Bitoun E, Bodemer C, Amiel J, et al. Prenatal diagnosis <strong>of</strong> a<br />
lethal form <strong>of</strong> <strong>Netherton</strong> <strong>syndrome</strong> by SPINK5 mutation<br />
analysis. Prenat Diagn 2002; 22: 121–126.<br />
25 Bitoun E, Chavanas S, Irvine AD, et al. <strong>Netherton</strong> <strong>syndrome</strong>:<br />
Disease expression and spectrum <strong>of</strong> SPINK5 mutations in 21<br />
families. J Invest Dermatol 2002; 118: 352–361.<br />
26 Magert HJ, Standker L, Kreutzmann P, et al. LEKTI, A novel<br />
15-domain type <strong>of</strong> human serine proteinase inhibitor. J Biol<br />
Chem 1999; 274: 21499–21502.<br />
27 Sprecher E, Chavanas S, DiGiovanna JJ, et al. The spectrum<br />
<strong>of</strong> pathogenic mutations in SPINK5 in 19 families with<br />
<strong>Netherton</strong> <strong>syndrome</strong>: Implications for mutation detection<br />
and first case <strong>of</strong> prenatal diagnosis. J Invest Dermatol 2001;<br />
117: 179–187.<br />
28 Raghunath M, Tontsidou L, Oji V, et al. SPINK5 and<br />
<strong>Netherton</strong> Syndrome: novel mutations, demonstration <strong>of</strong><br />
missing LEKTI, and differential expression <strong>of</strong><br />
transglutaminases. J Invest Dermatol 2004; 123: 474–483.<br />
29 Suga Y, Tsuboi R, Hashimoto Y, et al. A case <strong>of</strong> Ichthyosis<br />
linearis circumflexa successfully treated with <strong>topical</strong><br />
<strong>tacrolimus</strong>. J Am Acad Dermatol 2000; 42: 520–522.<br />
30 Borzyskowski M, Grant DB, Wells RS. Cushing’s <strong>syndrome</strong><br />
induced by <strong>topical</strong> steroids <strong>use</strong>d for the treatment <strong>of</strong> nonbullous<br />
ichthyosiform erythroderma. Clin Exp Dermatol<br />
1976; 1: 337–342.<br />
31 Traupe H, Happle R. Etretinate therapy in children with<br />
severe keratinization defects. Eur J Pediatr 1985; 143: 66–<br />
69.<br />
32 Hausser I, Anton-Lamprecht I, Hartschuh W, et al.<br />
<strong>Netherton</strong>’s <strong>syndrome</strong>: ultrastructure <strong>of</strong> the active lesion<br />
under retinoid therapy. Arch Dermatol Res 1989; 281: 165–<br />
172.<br />
33 Godic A, Dragos V. <strong>Successful</strong> treatment <strong>of</strong> <strong>Netherton</strong>’s<br />
<strong>syndrome</strong> with <strong>topical</strong> calcipotriol. Eur J Dermatol 2004;<br />
14: 115–117.<br />
34 Nagata T. <strong>Netherton</strong>’s <strong>syndrome</strong> which responded<br />
to photochemotherapy. Dermatologica 1980; 161:<br />
51–56.<br />
35 Braun RP, Ramelet AA. Failure <strong>of</strong> cyclosporine in<br />
<strong>Netherton</strong>’s Syndrome. Dermatology 1997; 195: 75.<br />
36 Buxman M, Hickman J, Ragsdale W, et al. Therapeutic<br />
activity <strong>of</strong> lactate 12% lotion in the treatment <strong>of</strong> ichthyosis.<br />
Active versus vehicle and active versus a petrolatum cream.<br />
J Am Acad Dermatol 1986; 15: 1253–1258.<br />
37 Smith DL, Smith JG, Wong SW, et al. <strong>Netherton</strong>’s<br />
<strong>syndrome</strong>: a <strong>syndrome</strong> <strong>of</strong> elevated IgE and characteristic<br />
skin and hair findings. J Allergy Clin Immunol 1995; 95:<br />
116–123.<br />
38 Marsland AM, Griffiths CE. The macrolide<br />
immunosuppressants in dermatology: mechanisms <strong>of</strong><br />
action. Eur J Dermatol 2002; 12: 618–622.<br />
39 Gupta AK, Adamiak A, Chow M. Tacrolimus: a review <strong>of</strong> its<br />
<strong>use</strong> for the management <strong>of</strong> dermatoses. J Eur Acad Dermatol<br />
Venereol 2002; 16: 100–114.<br />
40 Grassberger M, Steinh<strong>of</strong>f M, Schneider D, et al.<br />
Pimecrolimus an anti-inflammatory drug targeting the skin.<br />
Exp Dermatol 2004; 13: 721–730.<br />
© 2006 The International Society <strong>of</strong> Dermatology International Journal <strong>of</strong> Dermatology 2007, 46,<br />
290–294<br />
293
294 Case report Calcineurin inhibitors in <strong>Netherton</strong> <strong>syndrome</strong> Saif and Al-Khenaizan<br />
41 Graham-Brown RA, Grassberger M. Pimecrolimus: a review<br />
<strong>of</strong> pre-clinical and clinical data. Int J Clin Pract 2003; 57:<br />
319–327.<br />
42 Hoetzenecker W, Meingassner JG, Ecker R, et al.<br />
Corticosteroids but not pimecrolimus affect viability,<br />
maturation and immune function <strong>of</strong> murine epidermal<br />
Langerhans cells. J Invest Dermatol 2004; 122:<br />
673–684.<br />
43 Kalth<strong>of</strong>f FS, Chung J, Musser P, et al. Pimecrolimus does not<br />
affect the differentiation, maturation and function <strong>of</strong> human<br />
monocyte-derived dendritic cells, in contrast to<br />
corticosteroids. Clin Exp Immunol 2003; 133: 350–359.<br />
44 Panhans-Gross A, Novak N, Kraft S, et al. Human<br />
epidermal Langerhans’ cells are targets for the<br />
immunosuppressive macrolide <strong>tacrolimus</strong> (FK506). J<br />
Allergy Clin Immunol 2001; 107: 345–352.<br />
45 Queille-Roussel C, Paul C, Duteil L, et al. The new <strong>topical</strong><br />
ascomycin derivative SDZ ASM 981 does not induce skin<br />
atrophy when applied to normal skin for 4 weeks: a<br />
randomized, double-blind controlled study. Br J Dermatol<br />
2001; 144: 507–513.<br />
46 Billich A, Aschauer H, Aszòdi A, et al. Percutaneous<br />
absorption <strong>of</strong> drugs <strong>use</strong>d in atopic eczema: pimecrolimus<br />
permeates less through skin than corticosteroids and<br />
<strong>tacrolimus</strong>. Int J Pharmacol 2004; 269: 29–35.<br />
47 Ruzicka T, Assmann T, Homey B. Tacrolimus: the drug for<br />
the turn <strong>of</strong> the millennium? Arch Dermatol 1999; 135: 574–<br />
580.<br />
48 Mrowietz U, Wustlich S, Hoexter G, et al. An experimental<br />
ointment formulation <strong>of</strong> pimecrolimus is effective in<br />
psoriasis without occlusion. Acta Derm Venereol 2003; 83:<br />
351–353.<br />
49 Beljan G, Traupe H, Metze D, et al. Comel-<strong>Netherton</strong><br />
<strong>syndrome</strong> with bacterial super infection. Hautarzt 2003; 54:<br />
1198–1202.<br />
50 Oji V, Beljan G, Beier K, et al. Topical pimecrolimus: a novel<br />
therapeutic option for <strong>Netherton</strong> <strong>syndrome</strong>. Br J Dermatol<br />
2005; 153: 1067–1068.<br />
International Journal <strong>of</strong> Dermatology 2007, 46, 290–294 © 2006 The International Society <strong>of</strong> Dermatology



![التجربية الأولي [Read-Only] - KSU](https://img.yumpu.com/15502211/1/190x135/-read-only-ksu.jpg?quality=85)