Pericarditi
Pericarditi
Pericarditi

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
PERICARDITIS<br />
Summaries<br />
-Introduction ( Key words)<br />
-Definition?<br />
-Frequency?<br />
-Risk factors?<br />
-Clinical signs?<br />
-Etiology?<br />
-Non specific diagnosis?<br />
-Etiological diagnosis?<br />
-Treatment?<br />
-Evolution?<br />
-Complications?<br />
-Prevention?<br />
-State of the art?<br />
-Publication from IFR on subject ?<br />
-More information on subject?<br />
-Correspondent from l'IFR48<br />
Key words<br />
Pericardial effusion – Tamponade – Constrictive pericarditis-<br />
Hypothyroidism - Q fever
Definition of the syndrome<br />
Acute pericarditis is a syndrome caused by the inflammation of<br />
the pericardium, a sac composed of visceral and parietal layers<br />
separated by the pericardial cavity. Acute pericarditis can be<br />
dry, fibrinous or effusive, independent from its etiology, and may<br />
occur as an isolated entity or as a result of a systemic disease<br />
Detection and treatment of pericarditis remains a challenging<br />
problem and the aetiology is unknown in 40 to 85% of the<br />
cases. We have previously developed [1] a diagnostic strategy<br />
that recommends the systematic use of a combination of non<br />
invasive tests for the diagnosis of benign pericardial effusions.<br />
In addition, it allowed identifying two frequently under<br />
diagnosed causes in our area, Q fever [2,3] and<br />
hypothyroidism, both of which are easily treated. This strategy<br />
lead to a reduction in the number of pericarditis classified as<br />
idiopathic compared to a prescription based on selecting<br />
laboratory tests intuitively [4,5].<br />
For some patients pericardiocentesis is necessary. We perform<br />
a systematic analysis of pericardial fluid and biopsy specimens,<br />
using cultures and molecular analyses for identification of<br />
bacteriological, fungal, and viral agents, as well as<br />
histopathological examination [6].<br />
1/ Levy PY, Corey R, Berger P, et al. Etiologic diagnosis of 204<br />
pericardial effusions. Medicine (Baltimore) 2003; 82: 385-91.<br />
2/ Levy PY, Raoult D. Coxiella burnetii pericarditis : a report of<br />
15 cases and review. Clin Infect Dis. 1999;29:393-397.
3/ Levy PY, Thuny F, Habib G, Bonnet JL, Djiane P, Raoult D:<br />
Diagnosis of Coxiella burnetii pericarditis by using a<br />
systematic prescription kit in case of pericardial effusion. N Y<br />
Acad Sci. (in press 2006)<br />
4/ Levy PY, Moatti J.P, Gauduchon V, Vandenesch F, Habib G,<br />
Raoult D. comparison of intuitive versus systematic strategies<br />
for etiological diagnosis of pericardial effusion.. Scand J Infect<br />
Dis 2005; 37, 216-20.<br />
5/ Levy PY, Kahn M, Raoult D. Acute pericarditis. N Engl J<br />
Med 2005; 352:1154-5;<br />
6/ Levy PY, Fournier PE, Charrel R, Habib G, Metras, Raoult<br />
D: Molecular analysis of pericardial fluid: a 7 year experience.<br />
Eur Heart J. 2006;16:1942-46.
Frequency?<br />
It represents 2.5% of hospitalized patients in Cardiology. In<br />
Marseilles we can estimated the frequency around 30/100.000<br />
inhabitants. However, the true incidence and prevalence of<br />
pericarditis remains difficult to measure. The incidence of<br />
pericarditis in postmortem studies ranges from 1-6% , whereas<br />
it is diagnosed ante mortem in only 0.1% of hospitalized<br />
patients, and in 5% of emergency room patients that present<br />
with chest pain in the absence of myocardial infarction. In Africa,<br />
the incidence of tuberculous pericarditis is rising as direct result<br />
of HIV where 40-75% of patients with large pericardial effusion<br />
are infected with HIV. Pericardial effusion occurs in up to onethird<br />
of patients with myxoedema and it is detected clinically in<br />
up to 20% of uremic patients who require chronic dialysis. [1].<br />
1.Maisch B, Seferovic PM Ristic AD, and al. Guidelines on the<br />
diagnosis and management of pericardial diseases. The<br />
Taskforce on diagnosis and management of pericardial<br />
diseases of the European Society of cardiology. Eur Heart<br />
J. 2004 ;25:587-610.
Risk factors?<br />
The diminution of steroidal treatment or anticoagulant treatment<br />
can be responsible of exacerbation of pericardial effusion.<br />
Radiation injury to the heart is a significant complication of<br />
radiation therapy used in the treatment of breast carcinoma,<br />
Hodgkin’s disease and non-Hodgkin lymphoma [1],. It is<br />
dependent on the radiation dosage, the duration of therapy, the<br />
volume of heart included in the radiation field and anterior<br />
weighting of the radiation dose<br />
It has been reported following cardiac perforation by catheter<br />
and epicardial pacemaker implantation Cardiac tamponade is<br />
more frequent following valve surgery than coronary bypass<br />
grafting[2].<br />
1. Brosius FC, Waller BF, Roberts WC. Radiation heart<br />
disease. Analyses of 16 young (aged 15 to 33 years)<br />
necropsy patients who received over 3,500 rads to the<br />
heart. Am J Med. 1981;70:519-530<br />
2. Tsang TS, Enriquez-Sarano M, Freeman WK, and al.<br />
Consecutive 1127 therapeutic echocardiographically<br />
quided pericardiocenteses: clinical profile, practice<br />
patterns and outcomes spanning 21 years. Mayo Clin Proc<br />
2002; 77: 429-36
Clinical diagnosis?Clinical signs.<br />
• Progressive, frequently severe chest pain, generally worse<br />
when lying supine, relieved by sitting and might radiate to the<br />
neck, arms. Since the phrenic nerve crosses the pericardium,<br />
pericarditis is often responsible of pain to the trapezius<br />
muscle ridges.<br />
• Dyspnea worsened with decubitus dorsal.<br />
• Additional symptoms can be observed, particularly fever,<br />
cough, sputum production, and weight loss, but are generally<br />
related to underlying diseases.<br />
Physical examination<br />
•A pericardial friction rub is pathognomonic. The intensity vary<br />
quickly and it is best heard at the left sternal border at end of<br />
expiration with the patient leaning forward. It is audible<br />
throughout the respiratory cycle which makes the difference<br />
from pleural rub.<br />
TO LISTEN<br />
•http://www-sante.ujf-grenoble.fr/sante/CardioCD/cardio/<br />
chapitre/405.htm<br />
•Clinical signs in favor of tamponade (pulsus paradoxus)<br />
should be searched.
Etiology?<br />
Etiology<br />
Bacterial , fungal and<br />
parasites Infections<br />
Coxiella burnetii<br />
Incidence Western<br />
countries<br />
Etiological<br />
Diagnostic tools<br />
(material)<br />
Depend on country7% of Serology (serum)<br />
infectious pericarditis]<br />
Tuberculosis 4% (7% of tamponade) Culture, Molecular<br />
Biology (PE,PB)<br />
Gram negative rods, Staphylococci, S.pneumoniae Rare
Pericardial perforation (penetrating injury,<br />
oesophageal perforation), cardiac injury (surgery,<br />
percutaneous procedures)<br />
Diseases in adjacent<br />
structures<br />
Myocardial infarction, and postmyocardial<br />
syndrome<br />
aortic dissection, pneumonia, pulmonary<br />
embolism, empyema<br />
Association with other<br />
syndromes<br />
Inflammatory bowel disease, Loffler,<br />
syndrome, Stevens-Johnson syndrome,<br />
giant-cell aortitis, hypereosinophilic<br />
syndromes, acute pancreatitis<br />
1-3%<br />
5-10% cases<br />
Rare
Stade IV: Reversion of T wave to normal.<br />
In addition to this features, are frequently associated,<br />
depression of PR segment, sinus tachycardia and microvoltage.<br />
• Echocardiography<br />
The advent of echocardiography, an accurate noninvasive<br />
method for the detection of effusion, has clarified the definition<br />
and led standardizing effusion as a clear entity. It reveals the<br />
size: small (echo free space in diastole10mm posterior); or large (>20mm eventually with<br />
compression of the heart).<br />
Pericardial biopsy
•<br />
Pericardiocentesis is a life-saving procedure in decompensate<br />
cardiac tamponade and is indicated for effusions of greater than<br />
20 mm in diastole visualized by echocardiography, in urgency<br />
in case of tamponnade.<br />
Percutaneous pericardiocentesis can be guided by fluoroscopy,<br />
echocardiography, or a surgical approach and, in most cases,<br />
can be done safely and rapidly. Puncture of pericardial fluid<br />
should be proposed as a second line of investigation when<br />
serological tests are negative (including antinuclear antibodies<br />
and serum thyroid-stimulating hormone), except in the case of<br />
urgent drainage for tamponade. It can be also proposed when a<br />
neoplasm, tuberculosis, or infection are suspected. [2].<br />
1/ Feigenbaum H. Pericardial disease. In: Feigenbaum H,<br />
ed. Echocardioraphy. 5th ed. Lea & Febiger;<br />
1994:556-588<br />
2/ Gibbs CR, Watson RD, Singh SP, Lip GYH. Management<br />
of pericardial effusion by drainage: a survey of 10 year’s<br />
experience in a city centre general hospital serving a<br />
multiracial population. Postgrad Med J 2000;76:809-13<br />
Etiological diagnosis?
1/ Constitution of the kit (specific strategy of the IFR)<br />
• As soon as the diagnosis is made :<br />
o Blood cultures set aero and anaerobic<br />
o Sterile swabs for viral culture of pharynx<br />
o Viral serology : HIV, Hepatitis C, CMV, EBV,<br />
Enterovirus, Adenovirus<br />
o Bacterial serology : Coxiella, Bartonella, Rickettsia,<br />
Legionella, Mycoplasma, Chlamydia, Brucella<br />
o Toxoplasma<br />
o Thyroid Stimulating Hormone, Waaler –Rose,<br />
Antinuclear antibodies<br />
• H+1 Blood cultures set aero and anaerobic<br />
• J+3 Sterile swabs for viral culture of pharynx<br />
• J+15 2 ème same serological tests as J0<br />
• [link to FICHE DE RENSEIGNEMENTS ] :<br />
2/ Analyse des liquides (stratégie spécifique de l’IFR)<br />
• Culture:<br />
o Standard agar and shell vials<br />
o Mycobacteria<br />
• Viral culture :<br />
o Shell vials: BGM, Vero, MDCK,cellules diploïdes MRC5<br />
• Molecular analysis :<br />
o Bacteria 16S RNA ; 18S RNA ; Mycobacterium<br />
o Virus : Herpes consensus ; Enterovirus ; Parvovirus B19<br />
• Histological examination :<br />
Stained with May-Grünwald-Giemsa hematoxylin-eosinsaffron.<br />
Special stains were used for detection of fungi and<br />
bacteria, which included periodic acid-Schiff, Giemsa, Brown-<br />
Hopps tissue Gram, Grocott-Gomori methenamine silver, and<br />
Warthin-Starry stains.<br />
3/ Suggested decisional algorithm)<br />
•
Circumstances of diagnosis<br />
Systematic<br />
Acute<br />
Chronic<br />
Tamponade<br />
Echocardiography<br />
Pericardial<br />
Obvious cause<br />
Non obvious cause<br />
Volume>200cc or<br />
CT scanner<br />
Diagnosis<br />
compatible<br />
Levy PY, Lepidi H, Habib G, Collard F, Raoult D: Etiological<br />
diagnosis of pericardial effusion. Future Microbiology.<br />
STOP<br />
2006;1:229-39<br />
Systematic non invasive<br />
exploration: Serological tests,<br />
TSH ACAN, Viral cultures.<br />
No<br />
diagnosis or<br />
inefficacy of<br />
treatment<br />
Tumors markers<br />
Research of primitive<br />
cancer<br />
Pericardiocentesis<br />
- Standard Culture<br />
- Viral culture<br />
- Mycobacteria<br />
- Molecular biology<br />
(16SRNA, 18SRNA,<br />
Enterovirus, Herpes<br />
consensus)
Treatment?Symptomatic treatment with aspirin (up to 650<br />
mg every 4 hours) or nonsteroidal anti-inflammatory drugs<br />
are the mainstay treatment. Ibuprofen is generally preferred for<br />
its rare side-effects, favourable impact on the coronary flow, and<br />
the large dose range 300-800mg every 6-8 hours. It can be<br />
continued for days or weeks. Colchicine (0.5mgbid) added or<br />
as monotherapy also appears to be effective for the initial attack<br />
and the prevention of recurrences. Systemic corticosteroid<br />
therapy should be restricted to connective tissues, uremic<br />
pericarditis. It is contraindicated in case of infectious pericarditis<br />
except in patients with secondary tuberculous pericarditis as an<br />
adjunct to tuberculostatic treatment.<br />
Quelle est l’évolution du syndrome?<br />
Evolution depends from etiology: acute benign pericarditis<br />
generally resolves with 3 weeks. Tuberculosis and radiation<br />
therapy tends to be responsible of constrictive pericarditis.<br />
Possible complications?<br />
Possible complications of pericarditis include cardiac<br />
tamponade, in which the accumulation of fluids can cause<br />
severe compression, recurrent pericarditis with a symptom free<br />
interval, and pericardial constriction, in which an adherent<br />
pericardium restricts the diastolic filling of the heart. Chronic (>3
months) pericarditis includes effusive, adhesive and constrictive<br />
forms<br />
• Myopericarditis<br />
It is characterized frequently by atrial arrhythmias and elevation<br />
of cardiac biological markers. Pejorative evolution toward<br />
cardiac insufficiency can be noted.<br />
• Tamponnade<br />
It is the decompensate phase of cardiac compression caused<br />
by effusion accumulation and the increased intrapericardial<br />
pressure. It can be an surgical urgency.<br />
Clinically, heard sounds are distant, orthopnoea, cough,<br />
dysphagia with episodes of unconsciousness are observed.<br />
Arterial hypotension with pulsus paradoxus (decreased of<br />
systolic pressure with breath inspiration) is noted. In half of the<br />
cases, it is from neoplasm origin and need surgical drainage.<br />
• Constrictive pericarditis<br />
It is a rare but severe disabling consequence of the chronic<br />
inflammation.
The calcification is responsible of the diminution of the diastolic<br />
filling which can be diagnose in front of right cardiac<br />
insufficiency signs, and micro voltage on l’EKG. On<br />
echocardiography is note pericardial thickness with<br />
sometimes small pericardial effusion, and expansion of the right<br />
atrial.<br />
• Recurrent pericarditis.<br />
Recurrent pericarditis with a symptom free interval are noted in<br />
20 to 30% of cases. It is generally due to a common mistake<br />
with the use of too low dose of non steroidal anti-inflammatory<br />
doses to be effective or a dose to rapidly decreased. Correct<br />
NSAID regimens usually improve the symptomatology.<br />
How to prevent infections?
Since the etiologies are multiple, it is not possible to prevent<br />
pericardial effusion.<br />
State of research in pericarditis field?<br />
The remaining idiopathic pericarditis still represents a high<br />
percentage and may be due to uncultivable agents or to<br />
unknown immune mechanisms. Potential underlying genetic<br />
disorders have been also reported. Electron microscopy is not<br />
very developed yet because it is still expensive but it will be a<br />
very interesting tool for the diagnosis of viral pericarditis. In<br />
Africa, the impact of HIV infection on outcome in tuberculous<br />
pericarditis is the crucial point and will have to be studied in<br />
long-term works. Improving therapeutical management to<br />
avoided recurrence is also a very important objective for the<br />
next few years. The indications for intrapericardial<br />
administration of drugs will probably increase.<br />
Main publications from l’IFR on pericardial effusion<br />
1.Levy PY, Raoult D. Coxiella burnetii pericarditis : a report of<br />
15 cases and review. Clin Infect Dis. 1999;29:393-397.
2.Levy PY, Corey R, Berger P, et al. Etiologic diagnosis of<br />
204 pericardial effusions. Medicine (Baltimore) 2003; 82:<br />
385-91.<br />
3.Levy PY,. Fournier PE, Carta M, Raoult D. Pericardial<br />
effusion due to Bartonella Quintana in homeless man. J<br />
Clin Microbiol 2003;41:5291-93.<br />
4.Levy PY, Moatti J.P, Gauduchon V, Vandenesch F, Habib G,<br />
Raoult D. comparison of intuitive versus systematic<br />
strategies for etiological diagnosis of pericardial effusion..<br />
Scand J Infect Dis 2005; 37, 216-20.<br />
5.Levy PY, Kahn M, Raoult D. Acute pericarditis. N Engl J<br />
Med 2005; 352:1154-5;<br />
6.Levy PY, Fournier PE, Charrel R, Habib G, Metras, Raoult<br />
D: Molecular analysis of pericardial fluid: a 7 year<br />
experience. Eur Heart J. 2006;16:1942-46.<br />
7.Levy PY, Lepidi H, Habib G, Collard F, Raoult D: Etiological<br />
diagnosis of pericardial effusion. Future Microbiology.<br />
2006;1:229-39.<br />
8.Levy PY, Thuny F, Habib G, Bonnet JL, Djiane P, Raoult D:<br />
Diagnosis of Coxiella burnetii pericarditis by using a<br />
systematic prescription kit in case of pericardial effusion. N<br />
Y Acad Sci. (in press 2006).<br />
More information on the subject?<br />
• Savoia MC, Oxman MN. Myocarditis and pericarditis. In:<br />
Mandell GL, Bennet JE, Dolin R, Eds. Principles and
Practice of Infectious Diseases, 6th Edition ed. Philadelphia:<br />
Churchill Livingstone, 2004, p.1052-70.<br />
• Permanyer-Miralda G, Sagrista-Sauleda J, Soler-Soler J.<br />
Primary acute pericardial disease: a prospective series of<br />
231 consecutive patients. Am J Cardiol. 1985; 56: 623-30.<br />
• Corey GR, Campbell PT, Van Trigt P, et al. Etiology of large<br />
pericardial effusions. Am J Med. 1993; 95: 209-13.<br />
• Troughton R.W, Asher C.R, Klein A.L. <strong>Pericarditi</strong>s.Lancet<br />
2004; 363:717-27.<br />
•Tsang TS, Enriquez-Sarano M, Freeman WK, and al.<br />
Consecutive 1127 therapeutic echocardiographically quided<br />
pericardiocenteses: clinical profile, practice patterns and<br />
outcomes spanning 21 years. Mayo Clin Proc 2002; 77:<br />
429-36.<br />
•Nugue O, Millaire A, Porte H and al. Pericardioscopy in the<br />
etiologic diagnosis of pericardial effusion in 141 consecutive<br />
patients. Circulation 1996; 94: 1635-41.<br />
•Lange RA, Hillis LD. Acute pericarditis. N Engl J Med<br />
2004;351:2195-202 .<br />
Who to call at IFR48<br />
Dr Pierre –Yves LEVY<br />
Associated professor<br />
04 91 38 55 14<br />
PLEVY@mail.ap-hm.fr
Consultations :<br />
Sur rendez vous Vendredi matin<br />
Hôpital la Timone Laboratoire de microbiologie 1 er Etage<br />
Sur rendez vous mercredi matin<br />
Hôpital la Timone Département de cardiologie 10 ème Etage
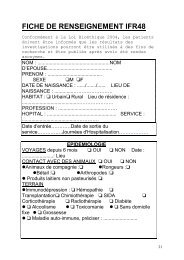
FICHE DE RENSEIGNEMENT IFR48<br />
Conformément à la Loi Bioéthique 2004, les patients<br />
ont été informés que sauf avis contraire de leur<br />
part, leurs prélèvements ou les résultats biologiques<br />
obtenus pourront être utilisés de manière anonyme à<br />
des fins scientifiques.<br />
NOM : .....................................................NOM<br />
D’EPOUSE................................................<br />
PRENOM : ........................................<br />
SEXE M F<br />
DATE DE NAISSANCE : ....../......./...... LIEU DE<br />
NAISSANCE : ..............……………………<br />
HABITAT : Urbain Rural Lieu de<br />
résidence : ..........................................…………………<br />
PROFESSION : ...................................…….<br />
HOPITAL : ...................................................<br />
SERVICE : .........................................………….<br />
Date d'entrée…………Date de sortie du service……………<br />
Journées d'Hospitalisation………………<br />
EPIDEMIOLOGIE<br />
VOYAGES depuis 6 mois OUI NON<br />
Date : .......................: Lieu<br />
CONTACT AVEC DES ANIMAUX OUI NON<br />
Animaux de compagnie : Rongeurs :<br />
Bétail : Arthropodes :<br />
Produits laitiers non pasteurisés <br />
TERRAIN<br />
Immunodépression : Hémopathie <br />
Transplantation Chimiothérapie SIDA<br />
<br />
Corticothérapie Radiothérapie Diabète<br />
Alcoolisme Toxicomanie Sans domicile<br />
fixe Grossesse<br />
Maladie auto-immune, préciser : .........................<br />
ANTECEDENTS<br />
Symptômes identiques à l’épisode actuel
Tuberculose Dysthyroïdie Cancer Exposition<br />
aux toxiques :<br />
CLINIQUE<br />
DATE DE DEBUT DES<br />
SYMPTOMES : ..................................<br />
CADRE NOSOLOGIQUE<br />
Péricardite aiguë Péricardite récidivante <br />
Myopéricardite Tamponnade<br />
Découverte échographique fortuite<br />
SYMPTOMES<br />
Fièvre Céphalées Syndrome pseudo-grippal<br />
Diarrhée Conjonctivite Pharyngite Uréthrite<br />
Arthrite Toux Adénopathies<br />
Eruption cutanée : Maculo-papuleuse <br />
Vésiculeuse Purpurique Erythème<br />
noueux<br />
Antibiothérapie préalable<br />
Frottement Douleurs rétro sternales<br />
Anomalies ECG <br />
Préciser : .............................................................................<br />
......<br />
Anomalies échocardiographiques <br />
Préciser : .........................................................................<br />
Anomalies radiologiques <br />
Préciser : .........................................................................<br />
BIOLOGIE<br />
Anomalies des leucocytes<br />
Hyperleucocytose à polynucléaires neutrophiles (><br />
10G/L)<br />
Hyperéosinophilie (> 500/mL)<br />
Leucopénie (< 1000/mL)<br />
Thrombopénie (< 150G/L)<br />
Elévation de la vitesse de sédimentation (> 20)<br />
Elévation des transaminases (> 1,5 N)<br />
Elévation de la créatinine (> 1,5 N)<br />
Elévation de la troponine (> 1,5 N)