UNIVERSITÀ DEGLI STUDI DI TRIESTE - OpenstarTs - Università ...
UNIVERSITÀ DEGLI STUDI DI TRIESTE - OpenstarTs - Università ...
UNIVERSITÀ DEGLI STUDI DI TRIESTE - OpenstarTs - Università ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
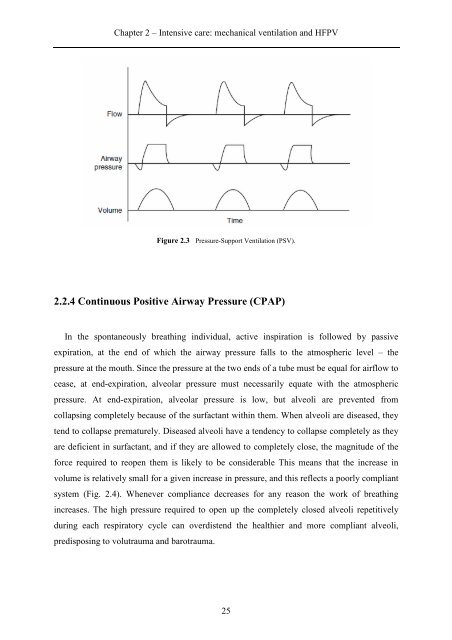
Chapter 2 – Intensive care: mechanical ventilation and HFPV<br />
Figure 2.3 Pressure-Support Ventilation (PSV).<br />
2.2.4 Continuous Positive Airway Pressure (CPAP)<br />
In the spontaneously breathing individual, active inspiration is followed by passive<br />
expiration, at the end of which the airway pressure falls to the atmospheric level – the<br />
pressure at the mouth. Since the pressure at the two ends of a tube must be equal for airflow to<br />
cease, at end-expiration, alveolar pressure must necessarily equate with the atmospheric<br />
pressure. At end-expiration, alveolar pressure is low, but alveoli are prevented from<br />
collapsing completely because of the surfactant within them. When alveoli are diseased, they<br />
tend to collapse prematurely. Diseased alveoli have a tendency to collapse completely as they<br />
are deficient in surfactant, and if they are allowed to completely close, the magnitude of the<br />
force required to reopen them is likely to be considerable This means that the increase in<br />
volume is relatively small for a given increase in pressure, and this reflects a poorly compliant<br />
system (Fig. 2.4). Whenever compliance decreases for any reason the work of breathing<br />
increases. The high pressure required to open up the completely closed alveoli repetitively<br />
during each respiratory cycle can overdistend the healthier and more compliant alveoli,<br />
predisposing to volutrauma and barotrauma.<br />
25