

Download the PDF - Optometry Today
Download the PDF - Optometry Today
Download the PDF - Optometry Today

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Some patients will attend clinical<br />
practice complaining of problems with<br />
near tasks such as reading or VDU work.<br />
This is usually due to a comitant<br />
deviation and, although troublesome<br />
because of <strong>the</strong> symptoms produced, <strong>the</strong>y<br />
are never life-threatening. However,<br />
patients may also attend with<br />
heterotropias. Whilst <strong>the</strong>se are usually<br />
long-standing deviations, patients may<br />
occasionally present complaining of<br />
sudden onset diplopia with unnoticed<br />
attendant heterotropia. The distinction<br />
between long-standing and recent onset<br />
heterotropia must be clearly made as<br />
acquired deviations usually indicate<br />
active pathology which can be lifethreatening.<br />
If not detected and<br />
adequately managed, <strong>the</strong>se may result in<br />
malpractice claims. In order to<br />
differentiate between such entities, a<br />
sound knowledge of <strong>the</strong> extraocular<br />
musculature and innervation is essential.<br />
BV FACTS<br />
Ten percent of all primary care patients<br />
exhibit a BV problem, and 2-3% of all<br />
subjects exhibit a heterotropia.<br />
Therefore, an optometrist that sees an<br />
average of 15 patients per day (75 per<br />
week), can expect approximately seven<br />
with a BV anomaly and one or two with<br />
a heterotropia.<br />
Lyndon Jones, BSc, PhD, FCOptom, DCLP, DOrth, Frank Eperjesi, BSc, MCOptom and<br />
Bruce Evans, BSc, PhD, FCOptom, DCLP<br />
Binocular vision evaluation in practice<br />
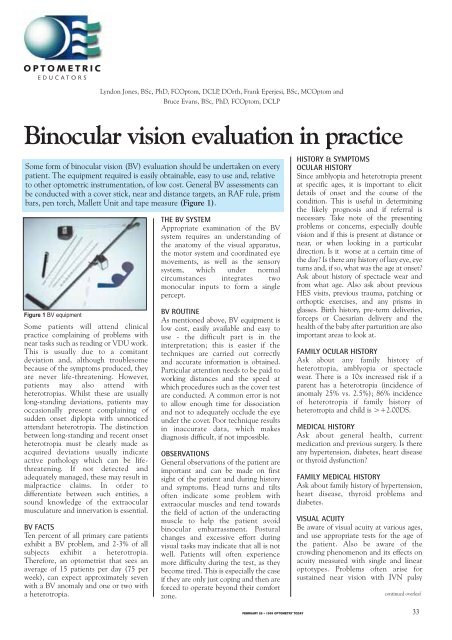
Some form of binocular vision (BV) evaluation should be undertaken on every<br />
patient. The equipment required is easily obtainable, easy to use and, relative<br />
to o<strong>the</strong>r optometric instrumentation, of low cost. General BV assessments can<br />
be conducted with a cover stick, near and distance targets, an RAF rule, prism<br />
bars, pen torch, Mallett Unit and tape measure (Figure 1).<br />
Figure 1 BV equipment<br />
THE BV SYSTEM<br />
Appropriate examination of <strong>the</strong> BV<br />
system requires an understanding of<br />
<strong>the</strong> anatomy of <strong>the</strong> visual apparatus,<br />
<strong>the</strong> motor system and coordinated eye<br />
movements, as well as <strong>the</strong> sensory<br />
system, which under normal<br />
circumstances integrates two<br />
monocular inputs to form a single<br />
percept.<br />
BV ROUTINE<br />
As mentioned above, BV equipment is<br />
low cost, easily available and easy to<br />
use - <strong>the</strong> difficult part is in <strong>the</strong><br />
interpretation; this is easier if <strong>the</strong><br />
techniques are carried out correctly<br />
and accurate information is obtained.<br />
Particular attention needs to be paid to<br />
working distances and <strong>the</strong> speed at<br />
which procedures such as <strong>the</strong> cover test<br />
are conducted. A common error is not<br />
to allow enough time for dissociation<br />
and not to adequately occlude <strong>the</strong> eye<br />
under <strong>the</strong> cover. Poor technique results<br />
in inaccurate data, which makes<br />
diagnosis difficult, if not impossible.<br />
OBSERVATIONS<br />
General observations of <strong>the</strong> patient are<br />
important and can be made on first<br />
sight of <strong>the</strong> patient and during history<br />
and symptoms. Head turns and tilts<br />
often indicate some problem with<br />
extraocular muscles and tend towards<br />
<strong>the</strong> field of action of <strong>the</strong> underacting<br />
muscle to help <strong>the</strong> patient avoid<br />
binocular embarrassment. Postural<br />
changes and excessive effort during<br />
visual tasks may indicate that all is not<br />
well. Patients will often experience<br />
more difficulty during <strong>the</strong> test, as <strong>the</strong>y<br />
become tired. This is especially <strong>the</strong> case<br />
if <strong>the</strong>y are only just coping and <strong>the</strong>n are<br />
forced to operate beyond <strong>the</strong>ir comfort<br />
zone.<br />
HISTORY & SYMPTOMS<br />
OCULAR HISTORY<br />
Since amblyopia and heterotropia present<br />
at specific ages, it is important to elicit<br />
details of onset and <strong>the</strong> course of <strong>the</strong><br />
condition. This is useful in determining<br />
<strong>the</strong> likely prognosis and if referral is<br />
necessary. Take note of <strong>the</strong> presenting<br />
problems or concerns, especially double<br />
vision and if this is present at distance or<br />
near, or when looking in a particular<br />
direction. Is it worse at a certain time of<br />
<strong>the</strong> day? Is <strong>the</strong>re any history of lazy eye, eye<br />
turns and, if so, what was <strong>the</strong> age at onset?<br />
Ask about history of spectacle wear and<br />
from what age. Also ask about previous<br />
HES visits, previous trauma, patching or<br />
orthoptic exercises, and any prisms in<br />
glasses. Birth history, pre-term deliveries,<br />
forceps or Caesarian delivery and <strong>the</strong><br />
health of <strong>the</strong> baby after parturition are also<br />
important areas to look at.<br />
FAMILY OCULAR HISTORY<br />
Ask about any family history of<br />
heterotropia, amblyopia or spectacle<br />
wear. There is a 10x increased risk if a<br />
parent has a heterotropia (incidence of<br />
anomaly 25% vs. 2.5%); 86% incidence<br />
of heterotropia if family history of<br />
heterotropia and child is >+2.00DS.<br />
MEDICAL HISTORY<br />
Ask about general health, current<br />
medication and previous surgery. Is <strong>the</strong>re<br />
any hypertension, diabetes, heart disease<br />
or thyroid dysfunction?<br />
FAMILY MEDICAL HISTORY<br />
Ask about family history of hypertension,<br />
heart disease, thyroid problems and<br />
diabetes.<br />
VISUAL ACUITY<br />
Be aware of visual acuity at various ages,<br />
and use appropriate tests for <strong>the</strong> age of<br />
<strong>the</strong> patient. Also be aware of <strong>the</strong><br />
crowding phenomenon and its effects on<br />
acuity measured with single and linear<br />
optotypes. Problems often arise for<br />
sustained near vision with IVN palsy<br />
continued overleaf<br />
FEBRUARY 26 • 1999 OPTOMETRY TODAY 33
Binocular vision evaluation in practice<br />
although distance vision is normal, so<br />
always carry out motility on those who<br />
complain of near vision problems (see<br />
later). With very young patients<br />
alternate occlusion can be used along<br />
with preferential looking, e.g. Keeler or<br />
Cardiff Acuity Cards. For older children,<br />
you can try matching pictures or shapes,<br />
e.g. Kay, Ffookes symbols, and for school<br />
age children Sheridan Gardiner,<br />
Sonksen-Silver or Glasgow Acuity Cards.<br />
COVER TEST<br />
This is a very important test as it can<br />
easily differentiate between a<br />
heterotropia and a heterophoria. It can<br />
also be used to estimate or measure <strong>the</strong><br />
direction and size of <strong>the</strong> deviation, and<br />
to give some indication whe<strong>the</strong>r it is<br />
compensated or not.<br />
Choose a suitable target in order to<br />
induce accommodation, do so slowly<br />
with good lighting. Cover, uncover,<br />
remove cover vertically and ensure <strong>the</strong><br />
eye is covered to avoid peripheral fusion<br />
locks. If amblyopia is suspected, take a<br />
little longer before removing <strong>the</strong> cover as<br />
<strong>the</strong> amblyopic eye requires longer to take<br />
up fixation. Decide if movements<br />
indicate a heterotropia, heterophoria or<br />
orthophoria, eso or exo, hypo or hyper.<br />
Estimate <strong>the</strong> size and speed of recovery<br />
and measure with a prism bar if you wish.<br />
Then do alternate cover and look for an<br />
increase size of deviation which is useful<br />
for small vertical deviations. Watch <strong>the</strong><br />
upper lids as any movement may indicate<br />
a vertical problem. Do not assume <strong>the</strong>re<br />
is no heterotropia if you see no<br />
movement; <strong>the</strong>re may be a microtropia<br />
with abnormal retinal correspondence so<br />
consider a four base-out prism test to<br />
determine if suppression is present.<br />
Figure 2 NPC assessment<br />
CONVERGENCE AMPLITUDE (NEAR<br />
POINT OF CONVERGENCE - NPC)<br />
This is only applicable for binocular<br />
patients and is particularly important for<br />
symptomatic exophores. It is important<br />
to choose an appropriate target, ei<strong>the</strong>r<br />
<strong>the</strong> dot and line on <strong>the</strong> RAF rule, or a<br />
near 6/9 letter, which is considered to be<br />
<strong>the</strong> clinical standard. It is absolutely<br />
inappropriate to use a pen-top. NPC is<br />
most accurately measured with <strong>the</strong> RAF<br />
rule, in <strong>the</strong> depressed position - 45<br />
degrees, and a slow speed (Figure 2).<br />
In order to check for fatigue it should<br />
be measured three times near <strong>the</strong><br />
beginning of <strong>the</strong> assessment and twice at<br />
<strong>the</strong> end. The value can be noted in terms<br />
of break (ei<strong>the</strong>r when <strong>the</strong> subject reports<br />
diplopia [subjective result] or when <strong>the</strong><br />
observer notices one or both eyes diverge<br />
[objective result]) and in terms of<br />
recovery (ei<strong>the</strong>r when <strong>the</strong> subject<br />
reports single vision or <strong>the</strong> observer<br />
notices that both eyes are pointing to <strong>the</strong><br />
test target). Both break and recovery are<br />
measured to <strong>the</strong> nearest half centimetre.<br />
A remote NPC with a break greater<br />
than 10cm is considered to be <strong>the</strong> most<br />
consistent finding in subjects with<br />
convergence insufficiency. Fatigue needs<br />
to be assessed as a subject may be able to<br />
produce one good result with <strong>the</strong> RAF<br />
rule, but <strong>the</strong> NPC may increase with<br />
fur<strong>the</strong>r testing. Many subjects report <strong>the</strong><br />
occurrence of symptoms only after<br />
several minutes of near point task<br />
performance.<br />
FUSIONAL RESERVES<br />
These (also called horizontal vergence<br />
reserves and prism vergences) can be<br />
measured in several ways. Orthoptists<br />
tend to use a prism bar (step vergence).<br />
Figure 3 Fusional reserves assessment<br />
Those optometrists with an interest in<br />
this field tend to use a Risley rotating<br />
prism (smooth vergence) ei<strong>the</strong>r<br />
monocularly in a trial frame, or<br />
binocularly in a phoropter. The results<br />
differ according to which procedure is<br />
used so, when making records, it is<br />
important to note <strong>the</strong> instrument used<br />
(Figure 3).<br />
Base-in and base-out values for near<br />
are usually <strong>the</strong> most useful although<br />
distance values can also be obtained.<br />
The blur, break and recovery points for<br />
both base directions need to be noted.<br />
This is a direct measure of <strong>the</strong> fusional<br />
vergence available to compensate for a<br />
phoria. The blur point is reached when<br />
<strong>the</strong> subject has used all <strong>the</strong>ir fusional<br />
reserves and has to use accommodative<br />
convergence to keep <strong>the</strong> test target<br />
single. As accommodative convergence<br />
is brought into play, <strong>the</strong> subject<br />
accommodates and <strong>the</strong> test target<br />
becomes blurred. The break point<br />
corresponds to <strong>the</strong> point when <strong>the</strong><br />
subject no longer has any fusional or<br />
accommodative vergence remaining and<br />
<strong>the</strong> test target becomes double.<br />
Norms are age-dependent. It is<br />
possible to have normal convergence<br />
amplitude as measured with <strong>the</strong> RAF<br />
rule push-up test and still have a<br />
vergence problem. This is known as<br />
fusional vergence dysfunction.<br />
AMPLITUDE OF ACCOMMODATION<br />
This is a measure of <strong>the</strong> maximum<br />
amount of accommodation an individual<br />
can exert and is usually measured using<br />
<strong>the</strong> RAF rule with <strong>the</strong> smallest text<br />
readable. It should be conducted<br />
monocularly and binocularly and<br />
repeated at least three times for each<br />
situation in order to assess for fatigue.<br />
This is important in esophores and<br />
symptomatic patients with NV problems.<br />
Ask <strong>the</strong> patient to read out loud <strong>the</strong><br />
smallest line <strong>the</strong>y can see, <strong>the</strong>n move <strong>the</strong><br />
target in and watch for saccades to make<br />
sure <strong>the</strong>y are accommodating on <strong>the</strong><br />
target; measure monocularly and<br />
binocularly and repeat to check for<br />
fatigue.<br />
ACCOMMODATIVE FACILITY<br />
This determines <strong>the</strong> speed of<br />
accommodative change. The dioptric<br />
accommodative stimulus is alternated<br />
between two different levels and <strong>the</strong><br />
subject reports when a letter target is<br />
seen clearly after each alternation in<br />
34<br />
FEBRUARY 26 • 1999 OPTOMETRY TODAY
Binocular vision evaluation in practice<br />
Figure 4 Accommodative facility assessment<br />
accommodative stimulus. The examiner<br />
counts <strong>the</strong> number of cycles completed<br />
in one minute (one cycle being <strong>the</strong><br />
change from one stimulus level to <strong>the</strong><br />
o<strong>the</strong>r and back again). Accommodative<br />
stimulus can be varied ei<strong>the</strong>r by lens<br />
power changes or by viewing distance<br />
changes. The first is referred to as lens<br />
rock and <strong>the</strong> second as distance rock,<br />
indicating that <strong>the</strong> accommodative<br />
stimulus is ‘rocked’ back and forth.<br />
The standard method of testing<br />
accommodative facility is a lens rock<br />
procedure using a pair of +2.00D lenses<br />
on one side of a flipper bar, and -2.00D<br />
lenses on <strong>the</strong> o<strong>the</strong>r side, although also<br />
available as ±1.00D and ±3.00D. The<br />
test is begun with <strong>the</strong> +2.00D lenses<br />
over <strong>the</strong> subject’s refractive correction.<br />
A test distance of 40cm is usually used<br />
with <strong>the</strong> reduced Snellen letters at a 6/6<br />
to 6/12 acuity demand for monocular<br />
testing (Figure 4). This type of target<br />
has no suppression control and it is more<br />
appropriate to use ei<strong>the</strong>r <strong>the</strong> Bernell<br />
vectogram SOV9 or <strong>the</strong> vertical fixation<br />
disparity bars on <strong>the</strong> near Mallett unit<br />
for binocular testing. Both need to be<br />
used with polarising filters.<br />
Some clinicians suggest that it may<br />
be more appropriate to train <strong>the</strong><br />
monocular accommodative facility prior<br />
to <strong>the</strong> binocular facility, especially if <strong>the</strong><br />
binocular lens rock performance is<br />
limited by fusional vergence dysfunction.<br />
Cut-offs for test failure using<br />
+2.00D/-2.00D flippers and a 40cm<br />
viewing distance for children and adults<br />
up to 30 years of age, are less than 11<br />
cycles per minute for monocular testing<br />
and less than 8 cycles per minute for<br />
binocular testing. Norms are agedependent.<br />
During binocular lens rock<br />
testing, adjustments in fusional vergence<br />
must occur to compensate for <strong>the</strong><br />
changes in accommodative vergence.<br />
Therefore, subjects may pass <strong>the</strong><br />
monocular lens rock but fail <strong>the</strong><br />
binocular lens rock facility if a vergence<br />
disorder is present.<br />
ACCOMMODATIVE LAG<br />
During accommodation for near-point<br />
viewing, <strong>the</strong> retina usually is conjugate<br />
with a point slightly behind <strong>the</strong> object of<br />
regard. For near-point targets,<br />
accommodative response is usually<br />
slightly less than <strong>the</strong> accommodative<br />
stimulus. The amount by which <strong>the</strong><br />
dioptric accommodative response is less<br />
than <strong>the</strong> dioptric accommodative<br />
stimulus is <strong>the</strong> lag of accommodation.<br />
This category of accommodation tests<br />
can be fur<strong>the</strong>r divided into: tests that<br />
measure <strong>the</strong> lag of accommodation; and<br />
tests in which lens power is changed to<br />
alter accommodative stimulus to <strong>the</strong><br />
point at which dioptric accommodative<br />
stimulus and dioptric accommodative<br />
response are equal.<br />
Monocular estimate method (MEM)<br />
dynamic retinoscopy is <strong>the</strong> procedure<br />
currently preferred by <strong>the</strong> authors. A test<br />
card with an aperture in <strong>the</strong> centre is<br />
used for dynamic retinoscopy so that <strong>the</strong><br />
examiner can observe <strong>the</strong> retinoscopic<br />
reflex close to <strong>the</strong> subject’s visual axis<br />
through <strong>the</strong> aperture. In MEM dynamic<br />
retinoscopy, <strong>the</strong> amount of <strong>the</strong> lag of<br />
accommodation is estimated by judging<br />
<strong>the</strong> width, speed and brightness of <strong>the</strong><br />
retinoscopic reflex. The test card and <strong>the</strong><br />
retinoscope are placed at <strong>the</strong> same<br />
distance from <strong>the</strong> subject’s spectacle<br />
plane, usually 40cm (Figure 5).<br />
With <strong>the</strong> retinoscope in <strong>the</strong> plane<br />
mirror mode, ‘with motion’ indicates a<br />
Figure 5 Accommodative lag assessment<br />
lag of accommodation and ‘against<br />
motion’ indicates a lead of<br />
accommodation. Neutrality indicates<br />
that <strong>the</strong> accommodative stimulus and<br />
accommodative response are equal. The<br />
examiner’s estimate of <strong>the</strong> amount of<br />
plus power that would be required to<br />
neutralise <strong>the</strong> ‘with motion’ is <strong>the</strong><br />
estimate of <strong>the</strong> lag of accommodation.<br />
The estimate of <strong>the</strong> lag can be confirmed<br />
by very briefly placing a plus lens equal in<br />
power to <strong>the</strong> estimated lag over one eye<br />
and quickly checking to see whe<strong>the</strong>r<br />
neutrality is observed. The lens should<br />
only be in place a half-second or less so<br />
that a change in accommodative<br />
response is not induced. School age<br />
children are reported to have a mean lag<br />
of +0.34D. Most non-presbyopic<br />
subjects have lags of 0 to +0.75D with<br />
MEM retinoscopy.<br />
MOTILITY<br />
To examine <strong>the</strong> action of a muscle and<br />
that of its yoke muscle, a motility test can<br />
be performed. In this test a pen-torch is<br />
moved in front of <strong>the</strong> subject in a star<br />
pattern, whilst <strong>the</strong> subject keeps <strong>the</strong>ir<br />
head and neck still. By moving <strong>the</strong> eyes<br />
in this manner, <strong>the</strong> maximal actions of all<br />
<strong>the</strong> extraocular muscles can be checked;<br />
<strong>the</strong> corneal reflexes should be observed.<br />
For example, <strong>the</strong> action of <strong>the</strong><br />
superior rectus (SR) muscle is best<br />
evaluated by placing <strong>the</strong> eye in an<br />
abducted position and checking <strong>the</strong><br />
degree of elevation, which can be<br />
achieved. Poor function of this muscle<br />
will be indicated by a reduced ability to<br />
elevate <strong>the</strong> eye in this abducted position<br />
and diplopia in <strong>the</strong> field of action of <strong>the</strong><br />
weakened muscle. The patient should be<br />
asked - “Is <strong>the</strong> double vision horizontal,<br />
vertical or oblique?” A cover test<br />
conducted in ‘up’ and ‘right’ gaze (in a<br />
case of a right SR weakness) will also<br />
show a hypotropia which is maximal in<br />
this position when compared with all<br />
o<strong>the</strong>r peripheral positions.<br />
Patients may present with ei<strong>the</strong>r a<br />
partial loss (paresis) or complete loss<br />
(paralysis) of muscle function. These<br />
terms are often used synonymously.<br />
Maximum and minimum fields of<br />
diplopia can be detected and an attempt<br />
made to try and isolate muscle or at least<br />
a pair of muscles. Alternatively, <strong>the</strong> eye<br />
with <strong>the</strong> outer most image has <strong>the</strong><br />
underacting muscle; images can be<br />
continued overleaf<br />
FEBRUARY 26 • 1999 OPTOMETRY TODAY 35
Binocular vision evaluation in practice<br />
enhanced by using red and green goggles.<br />
It is important to determine whe<strong>the</strong>r <strong>the</strong><br />
underaction is recent or long-standing<br />
and if <strong>the</strong> diplopia is sudden or of gradual<br />
onset. It should be noted that <strong>the</strong> vertical<br />
meridian is not a diagnostic direction of<br />
gaze, however, it is still useful to test in<br />
this direction, since it will help to identify<br />
A and V patterns more easily.<br />
EVALUATION OF BINOCULARITY<br />
(NON-HETEROTROPIC CASES)<br />
Fixation disparity is a technique familiar<br />
to most optometrists and will not be<br />
discussed in detail. The patient should be<br />
instructed to compare <strong>the</strong> position of <strong>the</strong><br />
green markers with and without <strong>the</strong><br />
Polaroid. Allow <strong>the</strong> patient to settle with<br />
<strong>the</strong> Polaroid and check that <strong>the</strong>y can see<br />
both markers, i.e. <strong>the</strong>y are not<br />
suppressing. Allow <strong>the</strong> patient to adapt<br />
by reading a line of text and <strong>the</strong>n<br />
neutralise any displacement with <strong>the</strong><br />
minimum prism - this is termed <strong>the</strong><br />
aligning prism, or small spheres. The<br />
displacement of <strong>the</strong> marker is referred to<br />
as fixation disparity. The markers may<br />
move back and forth across <strong>the</strong> neutral<br />
position indicating binocular instability;<br />
if <strong>the</strong> markers flicker this may be due to<br />
alternate suppression or retinal rivalry.<br />
ANTI-DIPLOPIA MECHANISMS<br />
Suppression is a negative adaptation to<br />
diplopia; it can vary in its intensity on a<br />
continuous scale from shallow to deep as<br />
well as in its size and position (ei<strong>the</strong>r<br />
central or peripheral). Central<br />
suppression can extend ten degrees from<br />
<strong>the</strong> fovea. Worth four-dots, stereoscope<br />
tests, Bagolini lenses and <strong>the</strong> Nonius bars<br />
on <strong>the</strong> Mallett unit can be used to detect<br />
suppression. The Mallett unit also has<br />
specific test words; some of <strong>the</strong> letters are<br />
seen by both eyes and some by only <strong>the</strong><br />
left or <strong>the</strong> right. They are of increasing<br />
size and allow a measure of <strong>the</strong> degree<br />
of suppression.<br />
ARC (abnormal retinal<br />
correspondence) which is almost<br />
always HARC and can be termed a<br />
positive adaptation to <strong>the</strong> heterotropia<br />
and is described as where<br />
correspondence exists between areas<br />
of <strong>the</strong> retina on <strong>the</strong> fixating and<br />
deviating eye which receive <strong>the</strong> same<br />
image. The correspondence prevents<br />
<strong>the</strong> occurrence of diplopia and allows<br />
for a limited degree of stereopsis. ARC<br />
is examined by <strong>the</strong> use of a Bagolini<br />
lens placed before <strong>the</strong> non-fixing eye<br />
while <strong>the</strong> patient is fixating a spot light<br />
target; if <strong>the</strong> patient reports <strong>the</strong> streak<br />
of <strong>the</strong> Bagolini lens as being centred<br />
on <strong>the</strong> spot, ARC may be diagnosed. A<br />
distance Mallett unit can be used; if<br />
<strong>the</strong> patient sees that <strong>the</strong> Nonius lines<br />
are aligned when a heterotropia is<br />
present, <strong>the</strong>re is ARC.<br />
ECCENTRIC FIXATION (MONOCULAR<br />
SENSORY ADAPTATION)<br />
This condition exists when a nonfoveal<br />
point is used for fixation; since<br />
retinal sensitivity is reduced<br />
parafoveally, <strong>the</strong>re is always a reduced<br />
acuity measured in <strong>the</strong>se eyes which<br />
depends upon <strong>the</strong> degree of<br />
eccentricity of fixation. Assessment<br />
can be made with <strong>the</strong> eccentric<br />
fixation graticule of <strong>the</strong> direct<br />
ophthalmoscope while occluding <strong>the</strong><br />
o<strong>the</strong>r eye; <strong>the</strong> target is usually red-free<br />
to ensure <strong>the</strong> patient remains<br />
comfortable during <strong>the</strong> test. The<br />
fixation can be classified according to<br />
its state (steady or unsteady), position<br />
(superior, inferior, nasal or temporal)<br />
and by its size in degrees from <strong>the</strong><br />
centre of <strong>the</strong> fixation target.<br />
Management of BV anomalies<br />
• Diagnosis of anomaly<br />
• Recent or long-standing?<br />
• Aetiology<br />
• Management<br />
• Referral or next review<br />
FURTHER READING<br />
1. Cashell, G.T.W. and Durran, I.M. (1980)<br />
‘Handbook of Orthoptic Principles 4th<br />
edition’. Churchill Livingstone, London.<br />
2. Stidwill, D. (1990) ‘Orthoptic Assessment<br />
and Management. Blackwell Science,<br />
London.<br />
3. Evans, B.J.W. (1997) ‘Binocular Vision<br />
Anomalies: Investigation and Treatment<br />
3rd edition’. Butterworth-Heinemann,<br />
Oxford.<br />
4. Scheimann, M. and Wick, B. (1994)<br />
‘Clinical Management of Binocular Vision,<br />
Heterophoric, Accommodative and Eye<br />
Movement Disorders’. Lippincott Raven,<br />
Philadelphia.<br />
5. Goss, D.A. (1995) ‘Ocular Accommodative,<br />
Convergence and Fixation Disparity. A<br />
Manual of Clinical Analysis 2nd edition’.<br />
Butterworth-Heinemann, Oxford.<br />
6. Birnbaum, M.H. (1993) ‘Optometric<br />
Management of Near-point Vision<br />
Disorders’. Butterworth-Heinemann,<br />
Oxford.<br />
7. Rowe, F. (1997) ‘Clinical Orthoptics’.<br />
Blackwell Science, London.<br />
USEFUL ADDRESSES<br />
For accommodative facility<br />
flipper bars without lenses, contact<br />
Paul Adler,<br />
50 High Street, Stotfold, Hitchin,<br />
Herts, SG5 4LL. Tel: 01462-732393<br />
Optometric Educators,<br />
PO Box 172, Bromley, Kent,<br />
BR2 OWZ. Tel: 0181-466 6535.<br />
Email: admin@optometrist.co.uk<br />
This is <strong>the</strong> second article in a<br />
series of five to be published, based on last<br />
September’s Optometric Educators<br />
lecture series entitled<br />
“Essential clinical skills for tomorrow’s patients”.<br />
36<br />
FEBRUARY 26 • 1999 OPTOMETRY TODAY













