

Chairside - Glidewell Dental Labs
Chairside - Glidewell Dental Labs
Chairside - Glidewell Dental Labs

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
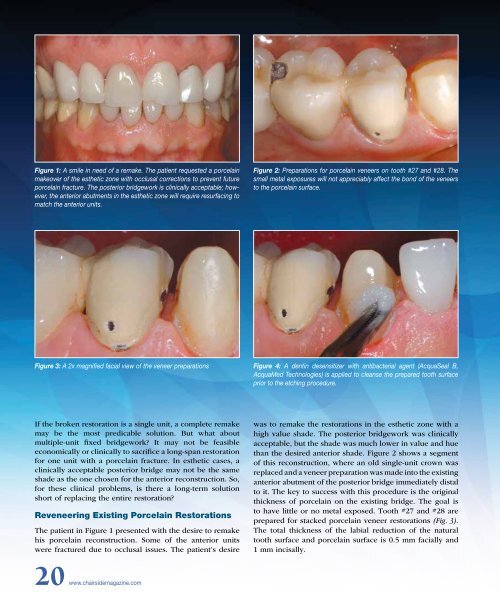
Figure 1: A smile in need of a remake. The patient requested a porcelain<br />
makeover of the esthetic zone with occlusal corrections to prevent future<br />
porcelain fracture. The posterior bridgework is clinically acceptable; however,<br />
the anterior abutments in the esthetic zone will require resurfacing to<br />
match the anterior units.<br />
Figure 2: Preparations for porcelain veneers on tooth #27 and #28. The<br />
small metal exposures will not appreciably affect the bond of the veneers<br />
to the porcelain surface.<br />
Figure 3: A 2x magnified facial view of the veneer preparations<br />
Figure 4: A dentin desensitizer with antibacterial agent (AcquaSeal B,<br />
AcquaMed Technologies) is applied to cleanse the prepared tooth surface<br />
prior to the etching procedure.<br />
If the broken restoration is a single unit, a complete remake<br />
may be the most predicable solution. But what about<br />
multiple-unit fixed bridgework? It may not be feasible<br />
economically or clinically to sacrifice a long-span restoration<br />
for one unit with a porcelain fracture. In esthetic cases, a<br />
clinically acceptable posterior bridge may not be the same<br />
shade as the one chosen for the anterior reconstruction. So,<br />
for these clinical problems, is there a long-term solution<br />
short of replacing the entire restoration?<br />
Reveneering Existing Porcelain Restorations<br />
The patient in Figure 1 presented with the desire to remake<br />
his porcelain reconstruction. Some of the anterior units<br />
were fractured due to occlusal issues. The patient’s desire<br />
was to remake the restorations in the esthetic zone with a<br />
high value shade. The posterior bridgework was clinically<br />
acceptable, but the shade was much lower in value and hue<br />
than the desired anterior shade. Figure 2 shows a segment<br />
of this reconstruction, where an old single-unit crown was<br />
replaced and a veneer preparation was made into the existing<br />
anterior abutment of the posterior bridge immediately distal<br />
to it. The key to success with this procedure is the original<br />
thickness of porcelain on the existing bridge. The goal is<br />
to have little or no metal exposed. Tooth #27 and #28 are<br />
prepared for stacked porcelain veneer restorations (Fig. 3).<br />
The total thickness of the labial reduction of the natural<br />
tooth surface and porcelain surface is 0.5 mm facially and<br />
1 mm incisally.<br />
20 www.chairsidemagazine.com













