

SHOT Annual Report 2009 - Serious Hazards of Transfusion
SHOT Annual Report 2009 - Serious Hazards of Transfusion
SHOT Annual Report 2009 - Serious Hazards of Transfusion

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Major Morbidity<br />
There was one patient that required venesection post transfusion.<br />
Case 3<br />
Entire adult unit <strong>of</strong> red cells given to infant<br />
A request was made for top-up transfusion for a sick 1-year-old child with an Hb <strong>of</strong> 9.0 g/dL. A dose <strong>of</strong> 110 mL was<br />
calculated and prescribed. An adult unit <strong>of</strong> blood was issued but nursing staff did not see the volume prescribed and<br />
transfused the entire unit <strong>of</strong> blood (230 mL). This transfusion took place between midnight and 08.00. The error was<br />
detected by laboratory staff when the patient’s post-transfusion Hb was 19 g/dL. The child required venesection.<br />
The reporting hospital stated that the prescription chart could be improved to allow clearer prescription for paediatric<br />
blood transfusion volumes. However, it is essential that all staff working in paediatrics are aware <strong>of</strong> the principles <strong>of</strong><br />
paediatric prescribing, based on body weight or surface area, whether administering blood components or pharmaceutical<br />
agents.<br />
Case 4 below describes the delayed and/or under-transfusion <strong>of</strong> a very anaemic neonate. It was thought that the<br />
prolonged anaemia may have contributed to long-term morbidity in this infant.<br />
Case 4<br />
Delay in transfusing very anaemic neonate has long term consequences<br />
A baby was delivered by CS and appeared unwell. There had been a massive transplacental haemorrhage and the<br />
infant’s Hb was 4 g/dL. The clinicians did not know this result until 2 hours post delivery. There was then a further<br />
delay <strong>of</strong> 4 hours before the baby was transfused, owing to misunderstandings and communication failures between<br />
clinicians, portering staff and the transfusion laboratory. The team did not seem to know that neonatal ‘flying squad’<br />
blood was available, nor did they ask for emergency blood even though the child was deteriorating. Blood was not<br />
prescribed. A sample was eventually sent but there were portering delays both in taking the sample and collecting the<br />
units. The total delay before transfusion commenced was over 4 hours. The baby became very sick and was transferred<br />
to a tertiary centre. There was long-term morbidity with developmental delay which may have been in part due to the<br />
prolonged period <strong>of</strong> extreme anaemia.<br />
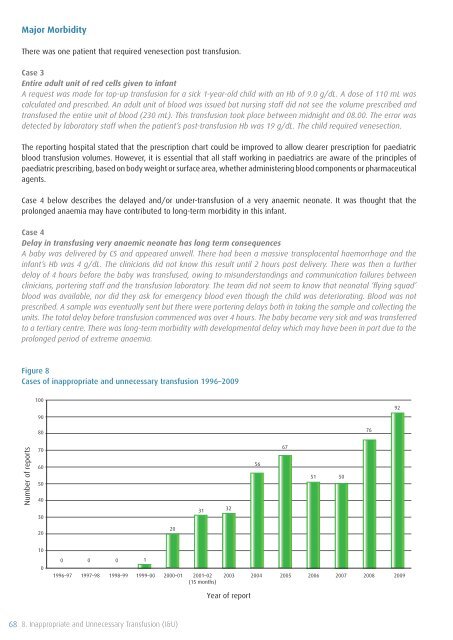
Figure 8<br />
Cases <strong>of</strong> inappropriate and unnecessary transfusion 1996–<strong>2009</strong><br />
100<br />
90<br />
92<br />
80<br />
76<br />
Number <strong>of</strong> reports<br />
70<br />
60<br />
50<br />
40<br />
30<br />
31<br />
32<br />
56<br />
67<br />
51 50<br />
20<br />
20<br />
10<br />
0<br />
0 0 0 1<br />
1996–97 1997–98 1998–99 1999–00<br />
2000–01<br />
2001–02<br />
(15 months)<br />
2003<br />
2004<br />
2005<br />
2006<br />
2007 2008 <strong>2009</strong><br />
Year <strong>of</strong> report<br />
68 8. Inappropriate and Unnecessary <strong>Transfusion</strong> (I&U)









