

SHOT Annual Report 2009 - Serious Hazards of Transfusion
SHOT Annual Report 2009 - Serious Hazards of Transfusion
SHOT Annual Report 2009 - Serious Hazards of Transfusion

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
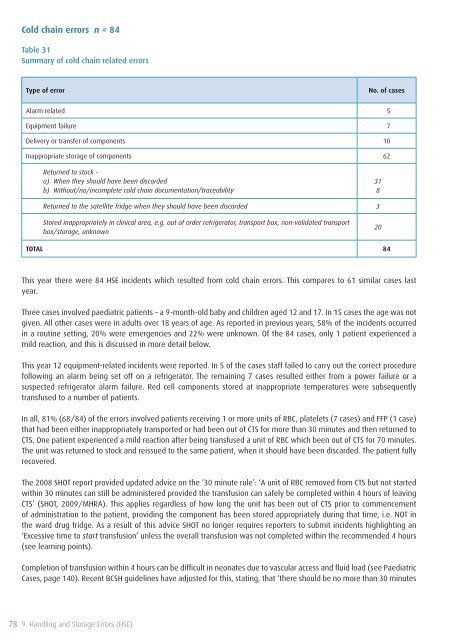
Cold chain errors n = 84<br />
Table 31<br />
Summary <strong>of</strong> cold chain related errors<br />
Type <strong>of</strong> error<br />
No. <strong>of</strong> cases<br />
Alarm related 5<br />
Equipment failure 7<br />
Delivery or transfer <strong>of</strong> components 10<br />
Inappropriate storage <strong>of</strong> components 62<br />
Returned to stock -<br />
a) When they should have been discarded<br />
b) Without/no/incomplete cold chain documentation/traceability<br />
31<br />
8<br />
Returned to the satellite fridge when they should have been discarded 3<br />
Stored inappropriately in clinical area, e.g. out <strong>of</strong> order refrigerator, transport box, non-validated transport<br />
box/storage, unknown<br />
20<br />
TOTAL 84<br />
This year there were 84 HSE incidents which resulted from cold chain errors. This compares to 61 similar cases last<br />
year.<br />
Three cases involved paediatric patients – a 9-month-old baby and children aged 12 and 17. In 15 cases the age was not<br />
given. All other cases were in adults over 18 years <strong>of</strong> age. As reported in previous years, 58% <strong>of</strong> the incidents occurred<br />
in a routine setting, 20% were emergencies and 22% were unknown. Of the 84 cases, only 1 patient experienced a<br />
mild reaction, and this is discussed in more detail below.<br />
This year 12 equipment-related incidents were reported. In 5 <strong>of</strong> the cases staff failed to carry out the correct procedure<br />
following an alarm being set <strong>of</strong>f on a refrigerator. The remaining 7 cases resulted either from a power failure or a<br />
suspected refrigerator alarm failure. Red cell components stored at inappropriate temperatures were subsequently<br />
transfused to a number <strong>of</strong> patients.<br />
In all, 81% (68/84) <strong>of</strong> the errors involved patients receiving 1 or more units <strong>of</strong> RBC, platelets (7 cases) and FFP (1 case)<br />
that had been either inappropriately transported or had been out <strong>of</strong> CTS for more than 30 minutes and then returned to<br />
CTS. One patient experienced a mild reaction after being transfused a unit <strong>of</strong> RBC which been out <strong>of</strong> CTS for 70 minutes.<br />
The unit was returned to stock and reissued to the same patient, when it should have been discarded. The patient fully<br />
recovered.<br />
The 2008 <strong>SHOT</strong> report provided updated advice on the ‘30 minute rule’: ‘A unit <strong>of</strong> RBC removed from CTS but not started<br />
within 30 minutes can still be administered provided the transfusion can safely be completed within 4 hours <strong>of</strong> leaving<br />
CTS’ (<strong>SHOT</strong>, <strong>2009</strong>/MHRA). This applies regardless <strong>of</strong> how long the unit has been out <strong>of</strong> CTS prior to commencement<br />
<strong>of</strong> administration to the patient, providing the component has been stored appropriately during that time, i.e. NOT in<br />
the ward drug fridge. As a result <strong>of</strong> this advice <strong>SHOT</strong> no longer requires reporters to submit incidents highlighting an<br />
‘Excessive time to start transfusion’ unless the overall transfusion was not completed within the recommended 4 hours<br />
(see learning points).<br />
Completion <strong>of</strong> transfusion within 4 hours can be difficult in neonates due to vascular access and fluid load (see Paediatric<br />
Cases, page 140). Recent BCSH guidelines have adjusted for this, stating, that ‘there should be no more than 30 minutes<br />
78 9. Handling and Storage Errors (HSE)









