SIMULATION CASEBOOK - MyCourses
SIMULATION CASEBOOK - MyCourses
SIMULATION CASEBOOK - MyCourses

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Gilbert Program in Medical Simulation<br />
Simulation Casebook<br />
Harvard Medical School Draft of the 1 st edition (2011), updated 3/2/12<br />
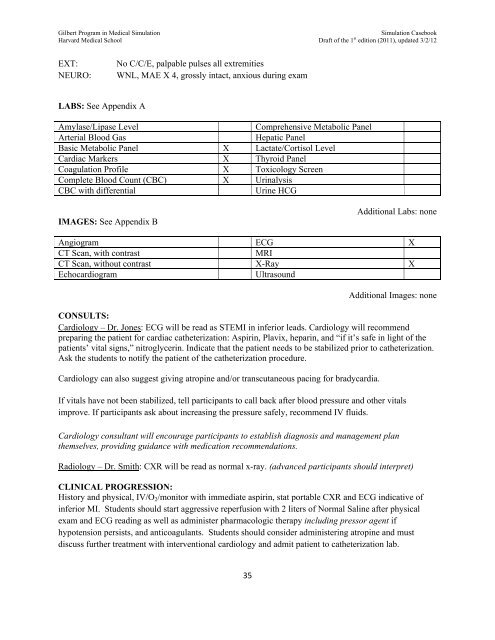
EXT:<br />
NEURO:<br />
No C/C/E, palpable pulses all extremities<br />
WNL, MAE X 4, grossly intact, anxious during exam<br />
LABS: See Appendix A<br />
Amylase/Lipase Level<br />
Arterial Blood Gas<br />
Basic Metabolic Panel X Lactate/Cortisol Level<br />
Cardiac Markers X Thyroid Panel<br />
Coagulation Profile X Toxicology Screen<br />
Complete Blood Count (CBC) X Urinalysis<br />
CBC with differential<br />
Urine HCG<br />
Comprehensive Metabolic Panel<br />
Hepatic Panel<br />
IMAGES: See Appendix B<br />
Additional Labs: none<br />
Angiogram ECG X<br />
CT Scan, with contrast<br />
MRI<br />
CT Scan, without contrast X-Ray X<br />
Echocardiogram<br />
Ultrasound<br />
Additional Images: none<br />
CONSULTS:<br />
Cardiology – Dr. Jones: ECG will be read as STEMI in inferior leads. Cardiology will recommend<br />
preparing the patient for cardiac catheterization: Aspirin, Plavix, heparin, and “if it’s safe in light of the<br />
patients’ vital signs,” nitroglycerin. Indicate that the patient needs to be stabilized prior to catheterization.<br />
Ask the students to notify the patient of the catheterization procedure.<br />
Cardiology can also suggest giving atropine and/or transcutaneous pacing for bradycardia.<br />
If vitals have not been stabilized, tell participants to call back after blood pressure and other vitals<br />
improve. If participants ask about increasing the pressure safely, recommend IV fluids.<br />
Cardiology consultant will encourage participants to establish diagnosis and management plan<br />
themselves, providing guidance with medication recommendations.<br />
Radiology – Dr. Smith: CXR will be read as normal x-ray. (advanced participants should interpret)<br />
CLINICAL PROGRESSION:<br />
History and physical, IV/O 2 /monitor with immediate aspirin, stat portable CXR and ECG indicative of<br />
inferior MI. Students should start aggressive reperfusion with 2 liters of Normal Saline after physical<br />
exam and ECG reading as well as administer pharmacologic therapy including pressor agent if<br />
hypotension persists, and anticoagulants. Students should consider administering atropine and must<br />
discuss further treatment with interventional cardiology and admit patient to catheterization lab.<br />
35