SIMULATION CASEBOOK - MyCourses
SIMULATION CASEBOOK - MyCourses
SIMULATION CASEBOOK - MyCourses

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Gilbert Program in Medical Simulation<br />
Simulation Casebook<br />
Harvard Medical School Draft of the 1 st edition (2011), updated 3/2/12<br />
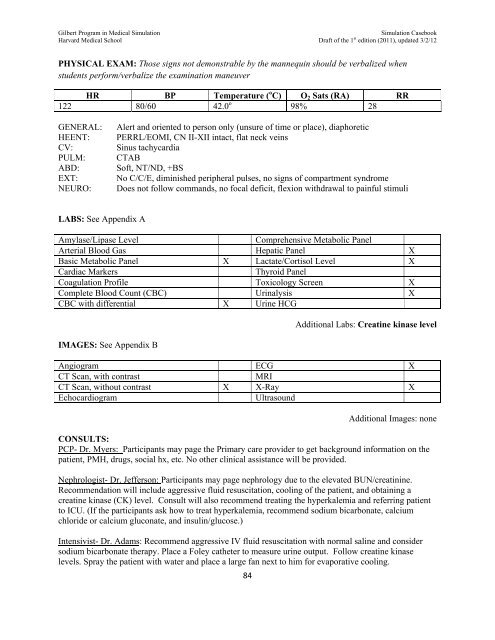
PHYSICAL EXAM: Those signs not demonstrable by the mannequin should be verbalized when<br />
students perform/verbalize the examination maneuver<br />
HR BP Temperature ( o C) O 2 Sats (RA) RR<br />
122 80/60 42.0 o 98% 28<br />
GENERAL:<br />
HEENT:<br />
CV:<br />
PULM:<br />
ABD:<br />
EXT:<br />
NEURO:<br />
Alert and oriented to person only (unsure of time or place), diaphoretic<br />
PERRL/EOMI, CN II-XII intact, flat neck veins<br />
Sinus tachycardia<br />
CTAB<br />
Soft, NT/ND, +BS<br />
No C/C/E, diminished peripheral pulses, no signs of compartment syndrome<br />
Does not follow commands, no focal deficit, flexion withdrawal to painful stimuli<br />
LABS: See Appendix A<br />
Amylase/Lipase Level<br />
Comprehensive Metabolic Panel<br />
Arterial Blood Gas Hepatic Panel X<br />
Basic Metabolic Panel X Lactate/Cortisol Level X<br />
Cardiac Markers<br />
Thyroid Panel<br />
Coagulation Profile Toxicology Screen X<br />
Complete Blood Count (CBC) Urinalysis X<br />
CBC with differential X Urine HCG<br />
IMAGES: See Appendix B<br />
84<br />
Additional Labs: Creatine kinase level<br />
Angiogram ECG X<br />
CT Scan, with contrast<br />
MRI<br />
CT Scan, without contrast X X-Ray X<br />
Echocardiogram<br />
Ultrasound<br />
Additional Images: none<br />
CONSULTS:<br />
PCP- Dr. Myers: Participants may page the Primary care provider to get background information on the<br />
patient, PMH, drugs, social hx, etc. No other clinical assistance will be provided.<br />
Nephrologist- Dr. Jefferson: Participants may page nephrology due to the elevated BUN/creatinine.<br />
Recommendation will include aggressive fluid resuscitation, cooling of the patient, and obtaining a<br />
creatine kinase (CK) level. Consult will also recommend treating the hyperkalemia and referring patient<br />
to ICU. (If the participants ask how to treat hyperkalemia, recommend sodium bicarbonate, calcium<br />
chloride or calcium gluconate, and insulin/glucose.)<br />
Intensivist- Dr. Adams: Recommend aggressive IV fluid resuscitation with normal saline and consider<br />
sodium bicarbonate therapy. Place a Foley catheter to measure urine output. Follow creatine kinase<br />
levels. Spray the patient with water and place a large fan next to him for evaporative cooling.