Document for PDF - Ministry of Health
Document for PDF - Ministry of Health
Document for PDF - Ministry of Health

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Improving<br />
Our <strong>Health</strong><br />
Te Whai Ora : Te Wero mo Aotearoa<br />
The Challenge <strong>for</strong> New Zealand
Mission Statement<br />
To allocate resources that secure the best health and independence<br />
<strong>for</strong> all New Zealanders.<br />
HFA Improving Our <strong>Health</strong> 1
Mihi (greetings)<br />
Tiheewa! Mauri! Ora,<br />
Ki nga tini aitua, nga mate huhua, mai I muri whenua,<br />
Tika tonu atu, ki te rerenga wairua haere, haere, haere<br />
Ki a tatou te hunga ora tena koutou<br />
Kia kaha tonu tatou ki te hapai I nga ahuatanga<br />
Katoa mo te iwi Maori ara nga iwi katoa o<br />
Aotearoa na reira kia u mai.<br />
Kia ora huihui mai ano tatou<br />
2
Foreword<br />
The <strong>Health</strong> Funding Authority has had the role since October 1998 <strong>of</strong> contracting,<br />
funding and monitoring public health services that the Government provides <strong>for</strong> the benefit<br />
<strong>of</strong> New Zealanders.<br />
From July this year the Government is introducing structural changes to the health sector<br />
that will widen the functions <strong>of</strong> the <strong>Ministry</strong> <strong>of</strong> <strong>Health</strong> to incorporate HFA functions, and<br />
establish District <strong>Health</strong> Boards. Though the planned change more appropriately reflects<br />
the Government’s vision <strong>for</strong> the health system, I feel that it is important to build on the<br />
substantial good work expert staff members within the HFA have been doing, and to<br />
acknowledge what they have achieved. I thank them <strong>for</strong> their ef<strong>for</strong>ts.<br />
I am pleased that this document, Improving Our <strong>Health</strong>: The Challenge For New Zealand,<br />
has been produced as an in<strong>for</strong>mation resource <strong>for</strong> the health sector. It outlines some <strong>of</strong> the<br />
issues and the exciting and innovative initiatives in Personal <strong>Health</strong> that the HFA has<br />
undertaken, and provides valuable and enlightening funding in<strong>for</strong>mation. The new District<br />
<strong>Health</strong> Boards, as they come on stream, will be able to build on much <strong>of</strong> the work done by<br />
the HFA.<br />
Meanwhile, I do not want to lose any <strong>of</strong> the momentum <strong>for</strong> improvement in the health<br />
arena and I look <strong>for</strong>ward positively to continuing those worthwhile partnerships that<br />
exist already.<br />
Hon Annette King<br />
Minister <strong>of</strong> <strong>Health</strong><br />
HFA Improving Our <strong>Health</strong> 3
Personal <strong>Health</strong><br />
Almost every New Zealander has used health services purchased by the Personal <strong>Health</strong><br />
operating group <strong>of</strong> the <strong>Health</strong> Funding Authority. General practitioners, midwives,<br />
laboratories, pharmacists, dentists, hospitals, hospices, nurse practitioners, and<br />
ambulance services are just some <strong>of</strong> the health care providers funded by Personal <strong>Health</strong><br />
on behalf <strong>of</strong> the Crown.<br />
Personal <strong>Health</strong> is the largest <strong>of</strong> the HFA’s operating groups, responsible <strong>for</strong> about twothirds<br />
($3.8 billion) <strong>of</strong> the HFA budget allocated to fund public health services. It comprises:<br />
the Service Strategy Team, the Change Management Team, and Locality Teams, who manage<br />
and contract health services in 11 Locality areas around the country.<br />
Personal <strong>Health</strong> Locality Teams have had a local focus within national frameworks, based<br />
in five HFA <strong>of</strong>fices: Auckland, Hamilton, Wellington, Christchurch, and Dunedin.<br />
They arrange most <strong>of</strong> the approximately 1100 health services contracts with the various<br />
health service providers. For example, the HFA has contracts and funding arrangements<br />
with doctors, independent Maori health providers, hospitals, laboratories, pharmacies<br />
and midwives.<br />
The Personal <strong>Health</strong> Service Strategy Team has developed national frameworks <strong>for</strong><br />
purchasing public health services to guide localities and ensure the public can get the<br />
same level <strong>of</strong> health service around the country. The Locality Team has assessed community<br />
needs and the effectiveness <strong>of</strong> local services as the basis <strong>of</strong> a Locality health plan.<br />
The Personal <strong>Health</strong> Change Management Team has ensured that changes to health services<br />
worked <strong>for</strong> the health sector, that the community could see the benefits, and that national<br />
change projects were implemented in a timely manner.<br />
This document, Improving Our <strong>Health</strong>: The Challenge <strong>for</strong> New Zealand, outlines the challenge<br />
that the Personal <strong>Health</strong> operating group <strong>of</strong> the HFA accepted and what has been done<br />
during the 1999 year to improve the health <strong>of</strong> New Zealanders, within the resources<br />
available, to fulfil the Crown’s health objectives. The HFA is required to provide in<strong>for</strong>mation<br />
to stakeholders. Here we <strong>of</strong>fer a snapshot <strong>of</strong>: health issues in the four main localities,<br />
issues <strong>of</strong> major focus, progress made working with the many health providers, and important<br />
clinical issues.<br />
The work <strong>of</strong> the Personal <strong>Health</strong> group, as a high per<strong>for</strong>mance organisation, has made a<br />
huge and positive difference to publicly-funded health services, by promoting innovation,<br />
equity, accountability, quality and integrity, and by valuing people.<br />
David Moore<br />
General Manager, Personal <strong>Health</strong><br />
4
Maori <strong>Health</strong><br />
As the Government moves to implement its change programme within the health sector,<br />
it is timely to reflect upon what the <strong>Health</strong> Funding Authority (HFA) has achieved in<br />
terms <strong>of</strong> Maori health. This document <strong>for</strong>ms part <strong>of</strong> that review.<br />
Clearly, the Personal <strong>Health</strong> group has been a major contributor to a rapidly growing<br />
awareness within the sector that Maori health needs are complex and substantial.<br />
Some <strong>of</strong> the complexities include the need to carefully select providers who are well<br />
equipped to deliver effective services to Maori. The quality <strong>of</strong> working relationships between<br />
the Personal <strong>Health</strong> and Maori <strong>Health</strong> groups <strong>of</strong> the HFA has contributed significantly to<br />
sound selections <strong>of</strong> a wide variety <strong>of</strong> capable providers.<br />
Moreover, the sharing <strong>of</strong> HFA resources between the various Operating Groups <strong>of</strong> the<br />
HFA, both <strong>of</strong> human and technological natures has provided a focused perspective on<br />
Maori health issues, which has helped to identify priorities. This focus on priorities has in<br />
turn called <strong>for</strong> innovative funding agreements to be developed with providers in ways<br />
which match Government’s policies.<br />
Some <strong>of</strong> those innovations are expanded upon later in this document.<br />
Also touched upon is the growing capacity <strong>of</strong> the HFA to identify gaps in services to<br />
Maori, particularly within what are <strong>of</strong>ten referred to as “mainstream services”. This growing<br />
capacity will become an essential feature <strong>of</strong> organisational competence within the public<br />
sector as Government policies on eliminating disparities and Maori developments become<br />
translated into action.<br />
Consequently, the experiences learnt in the HFA’s Personal <strong>Health</strong> Group, in regard to<br />
Maori health, are experiences which can contribute to the health sector as a whole, especially<br />
<strong>for</strong> the benefit <strong>of</strong> Maori.<br />
Rob Cooper<br />
General Manager, Maori <strong>Health</strong><br />
HFA Improving Our <strong>Health</strong> 5
In New Zealand every day...<br />
150 babies are born<br />
40,000 laboratory tests are analysed<br />
6800 outpatients visit hospitals <strong>for</strong> care<br />
460 people have surgical operations<br />
68,000 prescriptions <strong>for</strong> medicines are filled<br />
6
Contents<br />
Foreword 3<br />
Personal <strong>Health</strong> 4<br />
Maori <strong>Health</strong> 5<br />
The Challenge:<br />
Improving <strong>Health</strong> <strong>for</strong> all New Zealanders 8<br />
Localities: The Face <strong>of</strong> Personal <strong>Health</strong> 11<br />
Auckland Locality 11<br />
Hamilton Locality 12<br />
Wellington Locality 14<br />
South Island Locality Offices 15<br />
Our Focus 17<br />
Maori <strong>Health</strong>: Action Oriented Strategy 17<br />
Pacific Island <strong>Health</strong>:<br />
Growing and Young Population 18<br />
Child <strong>Health</strong>: High Levels <strong>of</strong> Activity 19<br />
Rural <strong>Health</strong>: Continual Focus 19<br />
Service Gaps: Being Addressed 20<br />
Working with Providers 21<br />
Hospitals: Purchasing Strategy<br />
and Issues 21<br />
Primary Care: Well Advanced 21<br />
Telephone Advice:<br />
A New Concept in New Zealand 22<br />
Pharmacy: Needs to Adapt 22<br />
Laboratory Contracts: Poised to<br />
Move Forward 23<br />
Maternity: Direction Correct but<br />
Improvements Required 23<br />
Clinical Issues and What We are Doing 27<br />
Waiting Times: Patient Focused Care 27<br />
Complex Medicine: Managing the Issue 29<br />
Diabetes: Moving Forward 29<br />
Asthma: a High Priority 30<br />
Heart Disease: Preparing the Way 30<br />
Oral <strong>Health</strong>: Focus on Youth 31<br />
Immunisations: Revamp in Action 32<br />
Hepatitis B: Screening Introduced 32<br />
Sexual and Reproductive Services:<br />
Under the Microscope 33<br />
Oncology: Reviewing Drugs<br />
and Radiation 33<br />
Palliative Care: Studied <strong>for</strong> the<br />
First Time 34<br />
Cervical Screening Investigation:<br />
Gisborne 34<br />
Paediatric Speciality Services:<br />
Review Underway 35<br />
Personal <strong>Health</strong> Financial In<strong>for</strong>mation 36<br />
Relationships With Communities 44<br />
Personal <strong>Health</strong> Senior<br />
Management Team 44<br />
Personal <strong>Health</strong> -<br />
External Advisory Groups and Committees 50<br />
Technical Working Groups within<br />
<strong>Health</strong> and Hospital Services 51<br />
<strong>Health</strong> - What’s Driving the Future 56<br />
Accident Insurance Re<strong>for</strong>m:<br />
Significant Risks 24<br />
Quality: Trans<strong>for</strong>ming the Sector 24<br />
HFA Improving Our <strong>Health</strong> 7
The Challenge:<br />
Improving <strong>Health</strong> <strong>for</strong> all New Zealanders<br />
The challenge to the HFA’s Personal <strong>Health</strong> group has been to improve health status within a given budget.<br />
The challenge is complicated - we cannot affect all <strong>of</strong> the determinants <strong>of</strong> health, we cannot do everything at<br />
once - but it has been important to us.<br />
Accepting this challenge required a mind shift from most <strong>of</strong> the activities <strong>of</strong> a health purchaser. For instance,<br />
in the days <strong>of</strong> the RHAs it was largely acceptable to contract <strong>for</strong> services, and manage to budget, without<br />
feeling responsible <strong>for</strong> outcomes. Implicit in accepting this challenge is that, in a very New Zealand way,<br />
there needed to be a fair chance <strong>for</strong> all and a need to focus resources where they would make the most<br />
difference.<br />
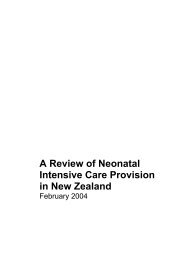
The biggest challenge is improving Maori health. Maori health is significantly under par - the table below<br />
dramatically shows the additional burden <strong>of</strong> disease carried by Maori, compared to the non-Maori population.<br />
Age Standardised DALY Rates <strong>for</strong> Cause Groups by Ethnicity<br />
Non Maori<br />
Maori<br />
Musculoskeletal<br />
Infection<br />
Infant peri-natal conditions<br />
Other chronic<br />
Endocrine<br />
Neurosensory<br />
Respiratory<br />
Injury<br />
Mental<br />
Cancer<br />
Cardio Vascular Disease<br />
0.0 10.0 20.0 30.0 40.0 50.0 60.0<br />
rate per 1,000<br />
Note: The Disability Adjusted Life Year (DALY) is a standardised Quality Adjusted Life Year (Qaly) type measure equal to the<br />
sum <strong>of</strong> Years Lost to Premature Mortality (YLL) and Years Lost to Disability (YLD).<br />
8
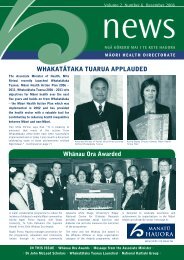
The increased mortality associated with the difference in health outcomes is demonstrated in the graph<br />
below. This graph is <strong>for</strong> the Wellington region but is broadly indicative <strong>of</strong> the pattern nation-wide.<br />
Proportion <strong>of</strong> Deaths Occurring at Different Ages in Wellington<br />
Residents 1990-94, by Gender and Ethnicity<br />
Maori Male<br />
Maori Female<br />
Non Maori Male<br />
Non Maori Female<br />
100%<br />
Proportion <strong>of</strong> Deaths 1990-94<br />
90%<br />
80%<br />
70%<br />
60%<br />
50%<br />
40%<br />
30%<br />
20%<br />
10%<br />
0%
Adoption <strong>of</strong> health outcome targets<br />
The fourth Labour Government introduced health outcome targets according to disease or high health<br />
risk behaviour.<br />
Personal <strong>Health</strong> has been implementing these measures. We accepted the targets and devolved the measures<br />
to localities, <strong>of</strong>f the back <strong>of</strong> the analytical work highlighted in the Wellington locality section, together with<br />
appropriate, revised budget measures. Work will continue measuring management per<strong>for</strong>mance against<br />
the targets.<br />
One set <strong>of</strong> targets is shown below, with comments on the trends.<br />
Target Indicator Target Level (year) Current Level Base Line Level<br />
(year)<br />
Future Trend<br />
Required<br />
Historical Trend<br />
Comment/Trend<br />
Hearing Loss<br />
Hearing Loss - all<br />
children<br />
Test failure rate at<br />
school entry<br />
5 percent (2000) 8.4 percent<br />
1996/97<br />
10.5 percent (1991) -12 percent pa -4 percent pa Tracking toward<br />
health but slow<br />
Hearing Loss -<br />
Maori children<br />
Test failure rate at<br />
school entry<br />
5 percent (2000) 13.0 percent<br />
1996/97<br />
14.8 percent (1991) -21 percent pa -3 percent pa Tracking toward<br />
health but slow<br />
Hearing Loss -<br />
Pacific children<br />
Test failure rate at<br />
school entry<br />
5 percent (2000) 16.1 percent<br />
1996/97<br />
14.0 percent (1991) -25 percent pa +3 percent pa Tracking away<br />
from health<br />
One <strong>of</strong> the major findings from attempting to apply this framework as an operational environment is the<br />
lack <strong>of</strong> timely, accurate in<strong>for</strong>mation.<br />
Extension <strong>of</strong> existing frameworks<br />
Our current work has been based on existing frameworks. The following is an example <strong>of</strong> how the table can<br />
be extended in the near future.<br />
Possible <strong>Health</strong> Indicators and Targets<br />
Indicators<br />
Targets<br />
Maori <strong>Health</strong><br />
Medical/Surgical<br />
Child <strong>Health</strong><br />
Separate reporting by ethnicity <strong>for</strong> all indicators listed below<br />
Reduction in:<br />
Maori smoking rates<br />
Maori asthma admissions<br />
Rate <strong>of</strong> maori low birth rate babies (
Localities : The Face <strong>of</strong> Personal <strong>Health</strong><br />
The community responsive arm <strong>of</strong> Personal <strong>Health</strong> has been organised in five locality <strong>of</strong>fices (with two in<br />
the South Island). These <strong>of</strong>fices are small (15 people in Auckland and in the South Island, 12 <strong>for</strong><br />
Wellington and Hamilton).<br />
They manage contracts <strong>for</strong> local needs by running the budget, managing relationships with communities<br />
and providers, and implementing change through nationally consistent contracting frameworks. Much <strong>of</strong><br />
the work has been done in moving to national consistency but less has been done in local innovation.<br />
There are notable positive exceptions, and all localities have dealt with issues in their own particular context.<br />
Auckland Locality<br />
Area served: Auckland, Northland<br />
Total population: 1.2 million<br />
Population Characteristics<br />
The Auckland localities include the poor rural<br />
Northland area and the large urban area <strong>of</strong> Auckland.<br />
• About a quarter (129,195) <strong>of</strong> all Maori live in the<br />
Auckland locality.<br />
• 80 percent <strong>of</strong> New Zealand’s Pacific Islands<br />
population lives in the Auckland locality.<br />
• The Auckland population is increasing at a faster<br />
rate than other parts <strong>of</strong> the country.<br />
• South Auckland has a high deprivation rating and<br />
poor health status<br />
• 72 percent <strong>of</strong> Maori in Counties Manukau live in<br />
the highest deprivation areas (deciles 8 -10).<br />
• 90 percent <strong>of</strong> Pacific Islands people in Counties<br />
Manukau live in the highest deprivation areas<br />
(deciles 8 -10).<br />
Specific Locality Issues<br />
Rapidly growing population and critical health status<br />
are the issues that most concern the Auckland locality.<br />
The critical situation in South Auckland has caught<br />
the attention <strong>of</strong> the public. Currently acute medical<br />
admissions are growing at 9 percent (the national<br />
average is 3 percent). Our team in Auckland has<br />
been working hard on solutions <strong>for</strong> both the short<br />
and the long-term. We expect to implement these<br />
initiatives in time <strong>for</strong> this year’s winter peak.<br />
The longer-term solution will take three to five years.<br />
Less visible, but equally critical, are issues in<br />
Northland. One example is its burgeoning need<br />
<strong>for</strong> dialysis services. There are many others. Our main<br />
focus has been to maintain and enhance the energy<br />
previously put into Northland by working with<br />
community groups, supporting Northland <strong>Health</strong><br />
and seeking innovative ways <strong>of</strong> getting to the needy<br />
(e.g. mobile clinics).<br />
Poor health is not just a Maori issue, but also a Pacific<br />
Islands one. Auckland has most <strong>of</strong> the country’s<br />
Pacific Islands peoples so most <strong>of</strong> our Pacific Islands<br />
team is based in Auckland.<br />
An example <strong>of</strong> the size <strong>of</strong> the issue is immunisation.<br />
Among two-year-olds with complete immunisation:<br />
tamariki Maori have a 45 percent immunisation rate,<br />
Pacific Islands children rate 53 percent, and 72 <strong>of</strong><br />
other children are immunised (last available figures<br />
are 1996).<br />
There is also considerable reshaping <strong>of</strong> hospital<br />
services in Auckland. Auckland <strong>Health</strong>care is<br />
constructing a new 710 acute bed tertiary facility<br />
and decreasing its secondary care. We are seeking<br />
to expand significantly (over the next 5 - 10 years)<br />
the range <strong>of</strong> secondary services delivered close to<br />
home on the North Shore and South Auckland,<br />
but particularly West Auckland. There is a great<br />
deal <strong>of</strong> tension between the three hospitals over<br />
the timing and size <strong>of</strong> the service adjustments.<br />
The Auckland <strong>of</strong>fice has been leading a significant<br />
project to help this adjustment.<br />
HFA Improving Our <strong>Health</strong> 11
Service projections 15 years <strong>for</strong>ward have been<br />
prepared by Personal <strong>Health</strong> to help in<strong>for</strong>m<br />
decisions around hospital configuration in the<br />
Auckland region.<br />
A major part <strong>of</strong> the Auckland locality’s work has<br />
been to build a positive relationship with providers.<br />
In particular, its predecessor (North <strong>Health</strong>) was<br />
known <strong>for</strong> its acrimonious relationships with<br />
primary care providers, mostly caused by differences<br />
in interpretation <strong>of</strong> the North <strong>Health</strong> primary care<br />
contract. Now, the Auckland <strong>of</strong>fice has almost all <strong>of</strong><br />
its primary care providers on the nationally<br />
consistent contract, and regular <strong>for</strong>ums are held with<br />
primary care providers to oversee development <strong>of</strong><br />
those contracts.<br />
Asian health is an emergent issue. The HFA<br />
contracts with Waitemata <strong>Health</strong> <strong>for</strong> Asian health<br />
support services to identify health care needs,<br />
provide access to health in<strong>for</strong>mation, provide<br />
in-service and meet the Asian community’s<br />
health needs.<br />
Major achievements <strong>for</strong> personal health in Auckland and Northland locality<br />
Better provider relationships<br />
Primary care dispute resolved<br />
Long-term contract with<br />
Auckland <strong>Health</strong>care<br />
Service reconfiguration<br />
Regional Trauma Centre<br />
Northland Rural GP Consortium<br />
Plunket services<br />
Pacific Islands health<br />
The HFA established better relationships with primary care organisations and hospitals,<br />
greatly enhancing opportunities <strong>for</strong> increasing the role <strong>of</strong> primary care providers in<br />
prevention and management <strong>of</strong> chronic and acute diseases.<br />
Settled a long outstanding major claim from previous administration regarding ProCare’s<br />
claim <strong>for</strong> settlements under budget share arrangements. Agreement by ProCare to<br />
implement a programme <strong>for</strong> Pacific Islands peoples was a significant outcome <strong>of</strong> the<br />
negotiated settlement.<br />
Agreed to a 13-year contract with Auckland <strong>Health</strong>care, in which the HFA guarantees a<br />
decreasing revenue stream and Auckland <strong>Health</strong>care agrees to generate positive health<br />
or financial gains <strong>for</strong> the HFA.<br />
Moved paediatric neurosurgical services from Auckland Hospital to Starship.<br />
Moved dermatology from Auckland Hospital to Greenlane Hospital.<br />
15-year service projections described.<br />
Regional configuration process begun.<br />
Auckland Hospital established as regional trauma centre<br />
Developed to address locum coverage and Continuing Medical Education needs <strong>of</strong><br />
rural GPs.<br />
Extra funding allocated to provide WellChild facilitation and support services.<br />
The HFA developed new child health services, and funded a mobile hearing testing<br />
service in the Auckland.<br />
Hamilton Locality<br />
Area served: Waikato, Taranaki, Bay <strong>of</strong> Plenty<br />
Total population: 678,000<br />
Population Characteristics<br />
The Hamilton localities are characterised by:<br />
• Large sparsely populated areas.<br />
• A younger age structure than New Zealand as a<br />
whole, and a higher proportion <strong>of</strong> Maori than<br />
the national average.<br />
• Large proportions <strong>of</strong> families with young and<br />
school-aged children, a significant number<br />
headed by single parents.<br />
• Almost one-third <strong>of</strong> people aged over 65 live<br />
on their own.<br />
• Incomes within the region are lower than<br />
national average, indicating greater disparity<br />
between high and low incomes<br />
Specific Locality Issues<br />
Rural health is a key concern as 40 percent <strong>of</strong> the<br />
locality’s population live in communities <strong>of</strong> less<br />
than 10,000. There is a high proportion <strong>of</strong> Maori.<br />
12
The hospital network in this locality is highly<br />
efficient. <strong>Health</strong> Waikato operates a ‘hub and spoke’<br />
provider network with its four rural facilities<br />
(Thames, Tokoroa, Te Kuiti and Taumarunui) as<br />
the spokes, and Waikato Hospital the hub. <strong>Health</strong><br />
Waikato is the second largest hospital in<br />
New Zealand and represents 10 percent <strong>of</strong><br />
hospital funding. This hub and spoke ensures that,<br />
as far as possible, services are delivered where<br />
people live and all people have equitable access to<br />
specialist services.<br />
Thames Hospital has been in the spotlight with calls<br />
<strong>for</strong> a return to 24-hour, seven days a week surgery.<br />
The current service is 24 hours, five days a week.<br />
The HFA does not support a return to seven days,<br />
as the volume <strong>of</strong> cases from Thames admitted to<br />
Waikato over a weekend do not justify the increased<br />
costs.<br />
All hospitals in the region have made significant<br />
progress toward reducing waiting times through<br />
the booking system, becoming more efficient and<br />
reducing historical deficits.<br />
There have been substantial issues around the<br />
nature <strong>of</strong> primary care contracts from its<br />
predecessor, Midland RHA. In reviewing and<br />
modifying the contact relationships, we have<br />
preserved some <strong>of</strong> the very positive aspects and<br />
eliminated the negative.<br />
One good aspect is the extent <strong>of</strong> capitation.<br />
Capitation provides an incentive <strong>for</strong> doctors<br />
to manage themselves <strong>for</strong> the benefit <strong>of</strong><br />
their population, rather than just collecting<br />
fees <strong>for</strong> services. About 75 percent <strong>of</strong> all<br />
doctors in this region are capitated. The result <strong>of</strong><br />
capitation has been a change <strong>of</strong> practice to using<br />
nurses more and GPs less. We have continued to<br />
review and enhance the quality review<br />
programmes.<br />
The Hamilton <strong>of</strong>fice leads the renegotiations <strong>of</strong> the<br />
First <strong>Health</strong> contract. The contract is on a nationally<br />
consistent basis. Now, any surplus from managing<br />
pharmaceuticals can be measured, and applied to<br />
the purchase <strong>of</strong> health services, rather than being<br />
gathered as a private pr<strong>of</strong>it.<br />
Major <strong>Health</strong> achievements <strong>for</strong> personal health in Hamilton locality<br />
Essential dental care extended Meeting the needs <strong>for</strong> low-income adults over the entire region with more than 100<br />
dentists involved.<br />
New mobile dental service<br />
KidZNet<br />
Integrated child health pilots<br />
New Traditions - Rotorua<br />
Plunket WellChild services<br />
Abortion services<br />
Pharmaceuticals<br />
Catering <strong>for</strong> three new schools, and nearly 2000 children in the Western Bay area.<br />
S<strong>of</strong>tware development <strong>for</strong> child health in<strong>for</strong>mation service. It is a provider-driven, joint<br />
HFA project & due to go live in February 2000. There has been interest from South<br />
Auckland, Wellington, Taranaki and Dunedin child health groups and IPAs wanting to<br />
use KidZNet system.<br />
New Traditions is a national site and has successfully integrated primary and secondary<br />
services. It is looking at specific projects across primary and secondary services. Rotorua<br />
has all but one GP as part <strong>of</strong> one IPA, which makes this possible.<br />
Moving towards one single national contract that will allow dollars to move to where<br />
people chose to go <strong>for</strong> their WellChild. There are a significant number <strong>of</strong> new providers<br />
introduced into this service.<br />
Midland women can now obtain an abortion within the region, with the extension<br />
<strong>of</strong> the service at Waikato and Thames hospitals and a new service at Tokoroa Hospital<br />
this year.<br />
Personal <strong>Health</strong> contracted 32 community pharmacies to provide greater and userfriendlier<br />
access.<br />
$2 million increase in oncology Allocated an additional $2 million to <strong>Health</strong> Waikato <strong>for</strong> 1572 chemotherapy treatments<br />
and 5508 radiotherapy treatments, to meet increasing demand.<br />
Maori Development Organisation<br />
The Midland region has two Maori development organisations - Poutiri Trust (Bay Of<br />
Plenty) and Tui Ora (Taranaki) leading the way toward better service co-ordination,<br />
access and quality <strong>for</strong> Maori. The Midland region also has the highest number <strong>of</strong><br />
independent Maori providers reflecting higher population rations <strong>of</strong> Maori and iwi/<br />
hapu structures.<br />
HFA Improving Our <strong>Health</strong> 13
Wellington Locality<br />
Area served: Wellington, Manawatu, Wanganui,<br />
Hawkes Bay, Gisborne, and Wairarapa<br />
Total population: 821,619<br />
Population Characteristics<br />
The Wellington <strong>of</strong>fice serves a diverse set <strong>of</strong><br />
localities. It ranges from the urban, relatively<br />
well-<strong>of</strong>f Wellington City to rural, poor Tairawhiti.<br />
There are several populations with a high<br />
percentage <strong>of</strong> Maori.<br />
The Wellington population is generally wealthier<br />
and healthier than the national norm. There are<br />
pockets, however, <strong>of</strong> considerable poverty and poor<br />
health status. Within Hawkes Bay and Tairawhiti<br />
there are particular areas that have a lower health<br />
status, due to the high proportion <strong>of</strong> Maori.<br />
These include the East Coast (95 percent Maori)<br />
and Wairoa (58 percent Maori). There are a large<br />
number <strong>of</strong> rural health centres in areas with<br />
declining populations and decreasing client<br />
numbers.<br />
Specific Locality Issues<br />
The Wellington locality is most advanced with<br />
development <strong>of</strong> the analytical base <strong>of</strong> health<br />
services. The locality has completed, and seeks to<br />
consult on, a substantial review <strong>of</strong> its population’s<br />
health. The work is particularly comprehensive and<br />
takes health, and the costs <strong>of</strong> lack <strong>of</strong> health, down<br />
to the finest level <strong>of</strong> definition we have ever<br />
achieved. We are now almost able to tell the average<br />
health <strong>of</strong> a person depending on where they live.<br />
We expect this work, ‘Improving our <strong>Health</strong> in<br />
Wellington’ to be a substantial vehicle in guiding<br />
health purchasing.<br />
Specific hospital service issues include:<br />
• The Wellington area hospital plan <strong>for</strong> the<br />
Porirua/Kapiti Coast areas. Cabinet decisions<br />
regarding accident and emergency services at<br />
Porirua will cost an estimated extra<br />
$500,000 annually.<br />
• Hospital per<strong>for</strong>mance: <strong>Health</strong>Care Hawkes Bay<br />
(financial viability because <strong>of</strong> depreciation<br />
costs); Capital Coast <strong>Health</strong> (per<strong>for</strong>mance<br />
issues); and some small HHSs such as Wairarapa<br />
<strong>Health</strong> (clinical viability issues).<br />
• Rural hospital service issues need resolving in<br />
Horowhenua, Taihape, Wairoa and Raetihi<br />
regions.<br />
• We have ensured the viability <strong>of</strong> Capital<br />
Coast <strong>Health</strong> by contracting <strong>for</strong> higher<br />
prices beginning next year. This was done<br />
to facilitate the new hospital and help with<br />
the current financial situation <strong>of</strong> Capital<br />
Coast <strong>Health</strong>. The locality carries a $5 million<br />
risk next year, which should be covered from a<br />
re-allocation <strong>of</strong> money from the tertiary<br />
adjuster.<br />
The Government is scoping an integrated care<br />
initiative <strong>for</strong> the Porirua/Kapiti area. The initiative<br />
is being led by the MoH.<br />
Pacific Islands health services are being developed<br />
in the region and will continue to expand.<br />
There are six hospitals in this region. If a hospital<br />
network were devised from scratch it would<br />
probably have the same number, but with a different<br />
arrangement <strong>of</strong> services.<br />
14
Major achievements <strong>for</strong> personal health in Wellington locality<br />
Models <strong>of</strong> care pilot with Wellington<br />
IPA and Capital Coast <strong>Health</strong><br />
Dental health<br />
Primary Maori <strong>Health</strong><br />
Te Puia Springs<br />
Child health<br />
HHS financial solvency<br />
Medical/surgical initiatives<br />
An integrated sexual health service<br />
in the Wellington region<br />
Focus on chronic obstructive pulmonary disease and congestive heart failure - two major<br />
causes <strong>of</strong> acute medical admissions.<br />
The new mobile children’s dental service <strong>for</strong> the Wellington region is to start soon.<br />
Dental health promotion service in Wanganui, Wellington, Hawkes Bay, Tairawhiti<br />
and the Manawatu. Contracts with a range <strong>of</strong> providers including four Iwi contracts.<br />
An Oranga Niho contract <strong>for</strong> Maori teenagers and low income adults in the Hawkes<br />
Bay region.<br />
A primary medical service in the Wairarapa by a Maori provider<br />
Transfer <strong>of</strong> health services at Te Puia Springs to the local iwi based health provider,<br />
Ngati Porou Hauora.<br />
Provision <strong>of</strong> paediatric surgery outreach clinics.<br />
Development <strong>of</strong> child health facilitation and support services in Wanganui.<br />
Capital Coast <strong>Health</strong>, Good <strong>Health</strong> Wanganui and MidCentral <strong>Health</strong> are now on the<br />
road to solvency.<br />
Contract incentives <strong>for</strong> Capital Coast <strong>Health</strong> to work more closely with primary care<br />
organisations on the management <strong>of</strong> people with chronic diseases.<br />
Utilisation <strong>of</strong> Wairarapa <strong>Health</strong>’s spare capacity to provide general surgery operations.<br />
Significant reduction in waiting times <strong>for</strong> elective surgery at Hutt Valley <strong>Health</strong> and<br />
Wairarapa <strong>Health</strong>.<br />
Free access to young people between the ages <strong>of</strong> 19-25 with a community services card.<br />
South Island Locality Offices<br />
Area served: Nelson/Marlborough, Canterbury/<br />
Westland, Otago/Southland<br />
Total population: 899,472<br />
Population Characteristics<br />
• Most rural areas are slowly losing population<br />
• Dunedin, Christchurch (and its commuter belt),<br />
Nelson/Marlborough and the Wakatipu basin<br />
are growing. The West Coast is neither<br />
increasing nor decreasing.<br />
• Small rural population is scattered over vast<br />
territory meaning access problems.<br />
• Low Maori and Pacific Islands population.<br />
• Lower health status in inner cities and poor<br />
suburbs, the West Coast (especially Buller),<br />
and in some small rural towns.<br />
• There are more elderly in the South Island than<br />
other localities.<br />
Specific Locality Issues<br />
The South Island locality is characterised by<br />
declining population, other than Christchurch, but<br />
it covers a large regional area. This means the<br />
southern region faces different management<br />
problems. The region operates through two <strong>of</strong>fices,<br />
and manages a service budget that isn’t growing as<br />
fast as that <strong>of</strong> other <strong>of</strong>fices.<br />
There are substantial viability issues around rural<br />
hospitals. HHSs have signalled their wish to exit<br />
from at least two, possibly six, rural hospitals.<br />
The long-term viability <strong>of</strong> the newly established<br />
Central Otago Community Trust is an issue, as is<br />
the availability <strong>of</strong> some GP services in rural areas.<br />
West Coast, Nelson /Marlborough, Queenstown<br />
Lakes and Invercargill areas have economic scale<br />
problems because <strong>of</strong> their rural nature and small<br />
populations.<br />
An ageing population also poses challenges.<br />
There is increasing pressure to fund palliative care<br />
services more fully, reflecting a nation-wide trend.<br />
Further, there is growing pressure on the cost and<br />
HFA Improving Our <strong>Health</strong> 15
volume <strong>of</strong> community service, as more people leave<br />
hospital earlier and with more complex problems.<br />
In addition, acute medical volumes continue to<br />
grow faster than population, especially in<br />
Christchurch, particularly in respiratory, cardiology<br />
and general medical.<br />
The South Island has been wrestling with<br />
a significant budget problem. Personal <strong>Health</strong><br />
has a significant shortfall on purchasing<br />
emergency department attendances at <strong>Health</strong>care<br />
Otago and Southern <strong>Health</strong> ($1.3 million and<br />
$3 million).<br />
Christchurch is emerging as the major tertiary<br />
institution. Clinical viability <strong>of</strong> specific medical and<br />
surgical services (e.g. neurosurgery at <strong>Health</strong>care<br />
Otago, ophthalmology at Southern <strong>Health</strong>) is an<br />
issue, largely because <strong>of</strong> retention and recruitment<br />
<strong>of</strong> clinical staff in this area.<br />
Waiting times in surgical services are still high in<br />
some specialities.<br />
Major achievements <strong>for</strong> personal health in the South Island locality<br />
Pegasus contract<br />
Community trust contracts<br />
Emergency ambulance service<br />
<strong>for</strong> whole South Island<br />
New community hospice<br />
Director <strong>of</strong> Rural <strong>Health</strong><br />
Innovative support packages <strong>for</strong><br />
rural health centres<br />
Pacific Islands health service<br />
Integrated care project -<br />
Marlborough<br />
<strong>Health</strong> action plans<br />
An innovative contract including a project to manage acute demand growth.<br />
Put in place with new community trusts in the Waitaki, Central Otago, Gore and Balclutha<br />
areas, following the withdrawal <strong>of</strong> service provision by <strong>Health</strong>care Otago and Southern<br />
<strong>Health</strong>.<br />
A three-year emergency ambulance contract with the Order <strong>of</strong> St John close to finalisation,<br />
including delivery <strong>of</strong> the primary response in a medical emergency (PRIME) scheme to<br />
assist in provision <strong>of</strong> emergency services in geographically remote areas.<br />
Established by the Nelson Hospice Trust with the co-operation <strong>of</strong> Nelson Marlborough<br />
<strong>Health</strong>.<br />
Dr Pat Farry was appointed to this post earlier this year.<br />
The HFA has worked with district councils, health trusts and centres to locate new GPs,<br />
build a locum database and provide support packages and retain general medical and<br />
nurse practitioners.<br />
Additional child health funding was taken up by a new organisation, expanding services<br />
<strong>for</strong> the Pacific Islands community in Christchurch.<br />
The HFA is working with Marlborough <strong>Health</strong> Trust, the Nelson Marlborough <strong>Health</strong><br />
Services and the community on various projects to improve health services in the area.<br />
The HFA is working with South Link <strong>Health</strong> on developing diabetes and cardiovascular<br />
disease plans.<br />
16
Our Focus<br />
Maori <strong>Health</strong>: Action Oriented<br />
Strategy<br />
Issues<br />
Disparities in health status are a major concern and<br />
our focus is evident in the work being done in<br />
Maori health. We have been focusing on identified<br />
geographical areas (such as larger Maori populations<br />
with lower socio-economic status) and on particular<br />
service areas where Maori have poorer health.<br />
The total Maori population is 523,365 (nearly 15<br />
percent <strong>of</strong> the population). Some localities are<br />
densely populated by Maori where health status is<br />
particularly poor - notably Wairoa, South Auckland,<br />
East Coast, Hutt Valley, Northland, Bay <strong>of</strong> Plenty.<br />
Many <strong>of</strong> these areas also have significant rural<br />
health issues. Funding plans <strong>for</strong> these localities<br />
emphasise the higher numbers <strong>of</strong> Maori, who <strong>of</strong>ten<br />
have greater need <strong>for</strong> more appropriate services in<br />
a diversity <strong>of</strong> settings - marae, Maori health clinics,<br />
mobile services. Often the diversity <strong>of</strong> providers<br />
needs to be greater to promote choice and access<br />
so in these areas we have worked hard to ensure<br />
the number <strong>of</strong> Maori providers is greater.<br />
Our funding plan gives full regard to HFA Maori<br />
health policy <strong>of</strong>:<br />
• Greater Maori participation at all levels <strong>of</strong> the<br />
health sector<br />
• Mainstream enhancement<br />
• Maori Provider development<br />
Our projects place a heavy emphasis on Maori<br />
health gain and in particular the eight key priority<br />
areas identified and endorsed by the HFA Board.<br />
The key priority targets relevant to Personal <strong>Health</strong><br />
are: immunisation, diabetes, oral health, hearing<br />
and asthma. The choice <strong>of</strong> diabetes, asthma and<br />
oral health <strong>for</strong> disease management programmes<br />
was driven by these key priorities. Plans <strong>for</strong><br />
improvement in hearing and immunisation <strong>for</strong><br />
Maori are being driven through the child health<br />
strategy.<br />
We are acutely aware any plans <strong>for</strong> improving Maori<br />
health status must address the continuum <strong>of</strong> care -<br />
preventative programmes and improving access to<br />
primary and secondary care. This impacts on the<br />
way we fund and support preventative health<br />
education (with the Public <strong>Health</strong> group);<br />
the funding <strong>of</strong> primary care (GP services,<br />
pharmaceuticals, nursing services, sexual health,<br />
WellChild services); and the access and treatment<br />
<strong>of</strong> Maori in secondary care. We are seeking to<br />
increase Maori access to secondary care to ensure<br />
necessary treatment in some areas (complex<br />
diabetes treatment, cardiac surgery) but in others<br />
we are aiming to reduce hospitalisation (acute<br />
admissions <strong>for</strong> asthma).<br />
Personal <strong>Health</strong>’s Action<br />
All the plans developed integrate cultural factors<br />
that improve access, equity, effectiveness and<br />
ultimately health outcome. Examples <strong>of</strong> these<br />
include:<br />
Preventative Programmes<br />
• Supporting smokefree and smoking cessation<br />
initiatives (which impact on cancer, respiratory<br />
conditions, diabetes, heart disease, child health<br />
and life expectancy).<br />
• Increasing funding to Maori providers to<br />
provide education in nutrition, exercise, oral<br />
health, smoking cessation.<br />
• Ensuring programmes have implicit Maori<br />
health gain targets, such as the programmes <strong>for</strong><br />
Hepatitis B, breast screening, cervical screening,<br />
and diabetes.<br />
• Integrating health and education services with<br />
clinically based services.<br />
Primary Care Programmes<br />
• Integrating the role <strong>of</strong> Maori providers.<br />
• Development <strong>of</strong> funding <strong>for</strong>mulae which<br />
incorporate a measure <strong>of</strong> deprivation and<br />
ethnicity considerations.<br />
• Promoting better integration between IPAs,<br />
HHSs and Maori provider organisations,<br />
e.g. the Auckland <strong>Health</strong>care/Ngati Whatua<br />
joint venture <strong>for</strong> Hepatitis B screening<br />
• Supporting work<strong>for</strong>ce development to train<br />
Maori in key areas (child health, nurse<br />
educators).<br />
HFA Improving Our <strong>Health</strong> 17
Secondary Care Programmes<br />
• Ensuring Maori need is identified in an<br />
equitable way through Access Criteria <strong>for</strong><br />
surgery (Booking Systems project).<br />
• Identifying Maori utilisation <strong>of</strong> secondary care<br />
services and comparing this to prevalence <strong>of</strong><br />
disease in the population.<br />
• Paying a Maori <strong>Health</strong> Adjuster to hospitals to<br />
provide an incentive to improve service delivery<br />
to Maori, and contracting <strong>for</strong> quality measures<br />
with explicit Maori health requirements.<br />
Improving Access to Services<br />
• Family Start programme targeting Maori in key<br />
localities.<br />
• Maintaining the important role <strong>of</strong> Maori<br />
Community <strong>Health</strong> Workers and Support<br />
Workers in health care provision and advocacy<br />
<strong>for</strong> Maori whanau.<br />
• Ensuring Maori needs are met through<br />
telephone helplines (<strong>Health</strong>line, Plunketline,<br />
Maternity Helpline).<br />
• Improving the way in<strong>for</strong>mation is disseminated<br />
to Maori.<br />
Monitoring Service<br />
• Identifying and monitoring resource allocation<br />
<strong>for</strong> Maori.<br />
• Evaluating quality audit programmes measuring<br />
the effectiveness <strong>of</strong> services <strong>for</strong> Maori.<br />
In 1999/2000 Personal <strong>Health</strong> is reviewing<br />
maternity and child health services.<br />
• Collecting ethnicity data to support analysis <strong>for</strong><br />
decision making and resource allocation. This<br />
is a significant area <strong>for</strong> development through<br />
primary care, child health, immunisation and<br />
disease management projects. Currently we are<br />
able to report ethnicity specific in<strong>for</strong>mation <strong>for</strong><br />
most hospital services but the error rates (Maori<br />
recorded as non-Maori) in the figures produced<br />
can be as high as 50 percent in some hospitals.<br />
• Feedback and participation <strong>of</strong> Maori (at the<br />
levels <strong>of</strong> governance, provider and consumer)<br />
in projects provides direct evidence <strong>of</strong> service<br />
effectiveness. This will produce better<br />
outcomes <strong>for</strong> Maori. Involvement <strong>of</strong> Maori<br />
(both internal and external to the HFA) is a<br />
critical component <strong>of</strong> our methodologies in the<br />
process <strong>of</strong> shaping future-funding models.<br />
Pacific Island <strong>Health</strong>: Growing<br />
and Young Population<br />
Issues<br />
The estimated population <strong>of</strong> 227,000 (6 percent <strong>of</strong><br />
3.8 million) is young and diverse with a projected<br />
growth to 600,000 (12 percent <strong>of</strong> 4.8 million)<br />
by 2051. It comprises Samoan (50 percent),<br />
Cook Islands (22.5 percent), Tongan (15.5<br />
percent), Niuean (9.0 percent), Fijian (2.0 percent)<br />
and Tokelau (1.0 percent). Some 58 percent <strong>of</strong><br />
Pacific Islands resident in New Zealand in 1996<br />
were born in New Zealand. Some 80 percent <strong>of</strong> Pacific<br />
Islands people live in cities, mainly Auckland.<br />
Pacific Islands people <strong>of</strong>ten have lower health status<br />
than Maori with different behavioural patterns from<br />
the mainstream population, requiring a different<br />
approach. The four member HFA Pacific Islands<br />
health team is based in Auckland and Wellington.<br />
The socio-economic status <strong>of</strong> Pacific Islands people<br />
is low. The strategy ‘For Pacific by Pacific’ is based<br />
on these facts and the priority areas are: child and<br />
youth, maternity, primary care, and medium to<br />
long-term preventative health.<br />
Personal <strong>Health</strong>’s Action<br />
• In the past year new child services targeting<br />
Pacific Islands children have been purchased<br />
in Auckland, Wellington, Christchurch and<br />
Hastings. A mobile hearing testing service in<br />
Auckland (targeting Pacific Islands children)<br />
has been bought from the National Audiology<br />
Centre and has been operational since July<br />
1999. Child health and primary care services<br />
have been bought in Newtown (Wellington)<br />
and the Hutt. Provider organisations have been<br />
established in Christchurch, Hastings and<br />
Hamilton.<br />
• Joint ventures between Maori and Pacific<br />
Islands providers <strong>for</strong> services targeting children<br />
have been entered into in west and south<br />
Auckland, Porirua and the Hutt.<br />
• Multiple initiatives are aimed to produce benefit<br />
<strong>for</strong> the large numbers <strong>of</strong> Pacific Islands people<br />
in South Auckland.<br />
18
Child <strong>Health</strong>: High Levels <strong>of</strong><br />
Activity<br />
Issues<br />
New Zealand has one million children aged 14 or<br />
younger, with 57,000 babies born annually.<br />
Disparities <strong>of</strong> health outcome <strong>for</strong> Maori and Pacific<br />
Islands children are well documented. The Child<br />
<strong>Health</strong> Strategy (1998) and Strengthening Families<br />
Strategy provide the basis to address disparities and<br />
improve all children’s health.<br />
Personal <strong>Health</strong>’s Action<br />
Child <strong>Health</strong> In<strong>for</strong>mation System<br />
Quantitative in<strong>for</strong>mation on children’s health is not<br />
available in any easily retrievable <strong>for</strong>m.<br />
• Personal <strong>Health</strong> has been developing the Child<br />
<strong>Health</strong> In<strong>for</strong>mation Strategy (CHIS) which will<br />
be implemented progressively. Some aspects<br />
have already begun, such as the perinatal<br />
in<strong>for</strong>mation system and immunisation coverage<br />
(using HBL data)<br />
• The KidZNet pilot is underway, involving<br />
in<strong>for</strong>mation transfer between providers.<br />
This will govern the way a national in<strong>for</strong>mation<br />
system is established. National consistency will<br />
be ensured during implementation between<br />
providers and a range <strong>of</strong> systems.<br />
WellChild and Youth Service<br />
The key issues <strong>for</strong> WellChild are access and<br />
coverage.<br />
• A technical advisory group <strong>of</strong> clinicians,<br />
providers, and Personal <strong>Health</strong> is considering<br />
future directions <strong>for</strong> WellChild services,<br />
including the possible linkage <strong>of</strong> funding<br />
mechanisms <strong>for</strong> WellChild and immunisation<br />
services.<br />
• Integrated child health service approaches<br />
(facilitating co-ordination and in<strong>for</strong>mation<br />
sharing between providers) have been<br />
developed in West Auckland, Rotorua,<br />
Hamilton and Christchurch.<br />
• The development <strong>of</strong> a youth strategy focusing<br />
on sexual and reproductive health will<br />
commence in 2000.<br />
Family <strong>Health</strong> Initiatives<br />
Strengthening Families is a joint initiative to<br />
improve outcomes <strong>for</strong> children and young people<br />
at high risk. There are three programmes: Family<br />
Start, Local Co-ordination and Preventative<br />
Initiatives.<br />
• Personal <strong>Health</strong> is meeting regularly with<br />
health, education and social services policy staff<br />
to ensure effective national implementation.<br />
• Personal <strong>Health</strong> is the lead purchaser on a<br />
number <strong>of</strong> programmes. Four further<br />
programmes have been put in place by Personal<br />
<strong>Health</strong>.<br />
• In some areas there has been resistance to local<br />
co-ordination programmes. Personal <strong>Health</strong> is<br />
developing strategies accordingly.<br />
Rural <strong>Health</strong>: Continual Focus<br />
Issues<br />
Retention and recruitment <strong>of</strong> doctors in rural areas<br />
is one <strong>of</strong> the most significant problems facing the<br />
health sector. Rural communities, particularly<br />
small ones, have difficulty attracting and retaining<br />
health services. They can <strong>of</strong>ten support only one<br />
doctor who is constantly on call, isolated and has<br />
difficulty finding locums. The doctor-to-patient<br />
ratio in rural areas is lower than that <strong>of</strong> other areas.<br />
On-going pr<strong>of</strong>essional development is critical <strong>for</strong><br />
the safety <strong>of</strong> practice and to overcome pr<strong>of</strong>essional<br />
isolation.<br />
Rural communities have specific needs which must<br />
be taken into account: the disparity <strong>of</strong> health status<br />
<strong>of</strong> Maori; lower socio-economic groups; people<br />
with disabilities who require assistance; children<br />
and older adults; and the high injury rate.<br />
Access to services by Maori is a particular concern.<br />
For non-Maori, the rural health status measures<br />
compare favourably with urban.<br />
Personal <strong>Health</strong>’s Action<br />
We have developed initiatives over the past year to<br />
address these problems. These include:<br />
• Improving the retention <strong>of</strong> health pr<strong>of</strong>essionals<br />
through the change from the rural bonus to the<br />
rural ranking scheme; expansion <strong>of</strong> the Centre<br />
<strong>for</strong> Rural <strong>Health</strong> to a national role and the<br />
HFA Improving Our <strong>Health</strong> 19
funding <strong>for</strong> Rural Directors. In the North Island<br />
there is a specific requirement to <strong>for</strong>ge links and<br />
work to improve the health <strong>of</strong> Maori.<br />
• Developing appropriate skills and knowledge<br />
among rural pr<strong>of</strong>essionals to improve Maori<br />
health disparities, through modification and<br />
review <strong>of</strong> existing contracts.<br />
• Introducing the PRIME (Primary Response in<br />
a Medical Emergency) programme in the North<br />
Island to improve access to treatment in rural<br />
medical emergencies. This has involved funder<br />
collaboration (HFA and ACC) as well as<br />
provider (ambulance services, GPs and nurses)<br />
collaboration.<br />
• Encouragement and support <strong>of</strong> rural<br />
practitioners to develop networks and multidisciplinary<br />
teams to maximise the benefits <strong>of</strong><br />
the available resource.<br />
Service Gaps: Being Addressed<br />
Issues<br />
The budget bidding process, carried out in<br />
November, highlighted (to a greater level <strong>of</strong> detail)<br />
service gaps. Identifying these gaps and identifying<br />
a way to meet the needs <strong>of</strong> our people is a key<br />
challenge <strong>for</strong> Personal <strong>Health</strong>. Sometimes not<br />
meeting needs means waste and inefficiency as<br />
more is spent treating later. Often it means lost<br />
quality and quantity <strong>of</strong> life.<br />
The gaps that we have identified include:<br />
Immunisation <strong>of</strong> Maori and Pacific Islands Children<br />
Only 45 percent are currently immunised and it<br />
will require a 55 percent increase in funding to<br />
target the hard to reach. Existing contracts are not<br />
meeting demand.<br />
Medical Surgery<br />
Increased funding is required <strong>for</strong> emergency<br />
departments to reduce waiting times to acceptable<br />
levels. Increased oncology volumes has led to<br />
increased vascular surgery requirements. Radiology<br />
volumes need increasing. There is a shortfall in<br />
oncology radiation therapy. Renal and urology<br />
inpatient services need additional resources.<br />
Medical Surgery- elective<br />
Funding required to sustain level <strong>of</strong> elective surgery.<br />
Palliative Care<br />
Fully funding hospices.<br />
Laboratories<br />
Ensuring consistent pricing <strong>of</strong> outpatient<br />
laboratories across New Zealand.<br />
Maternity and Neo-natal<br />
Infertility services (including diagnostics).<br />
Oral <strong>Health</strong><br />
Dental services <strong>for</strong> low income adults. Increase in<br />
utilisation <strong>for</strong> children and adolescents. Dental<br />
education and examinations <strong>for</strong> pregnant women<br />
and mothers <strong>of</strong> pre-schoolers in at risk areas.<br />
Dental Brush-ins <strong>for</strong> pre-schoolers in at risk areas.<br />
Regional Inconsistency<br />
Regional inconsistencies also need addressing.<br />
Auckland funds sexual abuse services, Wellington<br />
does not. Auckland provides good access to<br />
infertility services, but they are poor elsewhere.<br />
Community referred radiology is restricted to<br />
Community Service Card holders in Wellington<br />
and the Hutt Valley. Insulin pumps are funded in<br />
some areas only. Some areas have no hospices, <strong>for</strong><br />
example the Midland region. Emergency dental<br />
services are not available in Hawkes Bay or the<br />
Hutt Valley.<br />
Personal <strong>Health</strong>’s action<br />
• We are prioritising what we can do with the<br />
available money. For instance, we are moving<br />
very quickly on some key immunisation issues<br />
(discussed below).<br />
• Medical surgery is being prioritised to those<br />
most in need, who can benefit from the surgery.<br />
• Clinical and service reviews are revealing some<br />
areas where substantial changes mean we can<br />
deliver more, <strong>for</strong> less money (eg. the developing<br />
dental strategy). Many <strong>of</strong> these issues are<br />
discussed further under clinical management.<br />
• We continue to identify gaps by mapping our<br />
service coverage document against locality<br />
contacts, by service reviews and by locality<br />
needs assessment.<br />
20
Working with Providers<br />
Hospitals: Purchasing Strategy<br />
and Issues<br />
Issues<br />
One <strong>of</strong> the biggest areas <strong>of</strong> our work ($3.2 billion<br />
from all operating groups) is shaping relationships<br />
with hospitals. The services provided are complex,<br />
significant and one <strong>of</strong> the traditional areas <strong>of</strong> service<br />
provision. The institutions are well resourced,<br />
complex and in considerably better order than a<br />
few years ago.<br />
Be<strong>for</strong>e Personal <strong>Health</strong> was established, the<br />
relationship between purchaser and provider was<br />
acrimonious, time consuming and negative.<br />
More recently issues about hospital purchasing<br />
strategy and issues have been debated and analysed<br />
in joint technical working groups be<strong>for</strong>e being<br />
escalated <strong>for</strong> policy decision making.<br />
Personal <strong>Health</strong>’s Action<br />
We have implemented ‘relationship contracting’.<br />
Both the HFA and hospitals explicitly recognise our<br />
interests are indelibly linked and are working<br />
together to achieve the wider goal <strong>of</strong> benefit to<br />
patients. We try to put our differences in a strategic<br />
contracting context, although there is significant<br />
tension <strong>for</strong> hospitals and purchaser to achieve their<br />
respective goals.<br />
In operational terms that means:<br />
• Evergreen contracts (lasting <strong>for</strong>ever) versus<br />
annual negotiations.<br />
• Continuous improvement <strong>of</strong> services (instead<br />
<strong>of</strong> once-<strong>of</strong>f, <strong>for</strong>ced changes).<br />
• Commitment to joint problem resolution and<br />
strategic planning.<br />
Some hospitals have found it easy to work in this<br />
environment. Others haven’t. Those that haven’t<br />
are <strong>of</strong>ten under considerable pressures, such as<br />
substantial capital investment programmes,<br />
which bring them up against ownership interests.<br />
In short, the sector is still learning to work in a<br />
co-operative way.<br />
The most controversial element is about money, as<br />
always. Hospitals are paid from a national price<br />
book that has prices <strong>for</strong> different types <strong>of</strong> operations<br />
described in a standard unit (called a cost weight).<br />
Important adjustments to the standard cost weight<br />
are payments <strong>for</strong> complexity (e.g. Starship) and<br />
payments <strong>for</strong> rurality (e.g. Wairarapa hospital).<br />
The sector faces important, unresolved questions:<br />
• Prices should be higher <strong>for</strong> mental health, lower<br />
<strong>for</strong> personal health<br />
• Capital costs should be included, but how<br />
• A price path should be paid, but at what level<br />
A significant further issue is the growth in acute<br />
medical volumes, an issue that needs to be resolved<br />
by primary care, but working in partnership with<br />
hospitals.<br />
Primary Care: Well Advanced<br />
Issues<br />
This is the public’s first point <strong>of</strong> contact with the<br />
health sector. The current delivery <strong>of</strong> care is based<br />
on an episodic approach responding to patient<br />
demands. There is an increasing demand on<br />
services, which have historically grown at 5 - 10<br />
percent annually, without demonstrable health<br />
gain. Technological advances, ageing population<br />
and shorter hospital stays are increasingly requiring<br />
a greater level <strong>of</strong> care.<br />
Primary care expenditure is $1.26 billion. Much <strong>of</strong><br />
this is indirect spending through referred services.<br />
In the current financial year Personal <strong>Health</strong> is<br />
<strong>for</strong>ecast to spend $631 million on pharmaceuticals,<br />
$251 million on General Practice subsidies<br />
(including practice nurses), $178 million on<br />
laboratory tests, $20 million on primary care<br />
organisation services, and $10.6 million on<br />
immunisation.<br />
There is a lack <strong>of</strong> co-ordinated and monitored care<br />
between providers - between hospital and primary<br />
care and between different primary care<br />
providers. Good in<strong>for</strong>mation is a key to addressing<br />
this issue.<br />
The HFA has agreement from the sector on<br />
specifications <strong>for</strong> shared in<strong>for</strong>mation. We regard<br />
this as a major accomplishment.<br />
HFA Improving Our <strong>Health</strong> 21
Privacy issues are significant. We plan to consult<br />
with the public on the increased use <strong>of</strong> National<br />
<strong>Health</strong> Indicator (NHI) on health data and<br />
appropriate processes to ensure privacy legislative<br />
obligations are met. The consultation is made up<br />
<strong>of</strong> three parts: 1) introducing NHI numbers onto<br />
all claims; 2) explaining to the public the purpose<br />
and use <strong>of</strong> ‘individual data’ (and in specific purposes<br />
when the HFA will have access to ‘identified’ data);<br />
3) the proposed processes to be used <strong>for</strong> the<br />
collection, storage and access <strong>of</strong> confidential patient<br />
in<strong>for</strong>mation.<br />
Personal <strong>Health</strong>’s Action<br />
Our gains in this area are well beyond what we<br />
believed possible.<br />
• Relationships with the sector have improved<br />
over the past year with the new focus on<br />
co-operation and openness. Almost all GPs in<br />
primary care organisations have moved to the<br />
new national contract.<br />
• The new national contracts provide <strong>for</strong> a<br />
consistent in<strong>for</strong>mation schedule, passive<br />
enrolment moving to active enrolment, crossmatching<br />
<strong>of</strong> registers and Maori quality<br />
standards (in other words, all the infrastructure<br />
to move to population based primary care).<br />
• Contracts with IPAs include action plans <strong>for</strong><br />
additional services, particularly <strong>for</strong> Maori.<br />
These will address areas <strong>of</strong> high health need or<br />
deliver important health outcomes.<br />
• Establishment <strong>of</strong> a joint working party to<br />
analyse issues relating to capitation.<br />
• A range <strong>of</strong> integration projects - Personal <strong>Health</strong><br />
has some 20 projects running with greater or<br />
lesser degrees <strong>of</strong> integration.<br />
We are consolidating on moves to greater national<br />
consistency:<br />
• Electronic claiming - by July 2000.<br />
• Internal Systems - making sure we can monitor<br />
and implement contract requirements.<br />
• NHI Implementation - <strong>for</strong> all claims, including<br />
ethnicity on General Medical Subsidy (GMS)<br />
and immunisation.<br />
A key issue is consultation on privacy <strong>of</strong><br />
in<strong>for</strong>mation issues. A work-stream is established<br />
and we are ready to discuss the issue.<br />
Telephone Advice: A New Concept<br />
in New Zealand<br />
Issues<br />
Telephone triage is a relatively new concept built<br />
on the system introduced by the United Kingdom<br />
Labour Government to the National <strong>Health</strong> Service<br />
(NHS). Telephone triage services assess the<br />
urgency <strong>of</strong> callers’ health problems and advise<br />
which service they should contact (such as<br />
ambulance, emergency department, GP, or selfcare)<br />
plus the appropriate timeframe within which<br />
this should be done. The intention is to reduce cost,<br />
by treating the matter over the telephone, and to<br />
reduce morbidity by getting those in need to GPs<br />
or emergency services faster.<br />
Patients are connected to the appropriate service<br />
and, with the patient’s agreement, can have the<br />
in<strong>for</strong>mation collected during the call <strong>for</strong>warded.<br />
The assessment and advice process are supported<br />
by a computer-based system designed to identify<br />
the cause <strong>of</strong> the complaint that is riskiest <strong>for</strong> the<br />
patient (rather than the most common or most<br />
likely cause).<br />
Personal <strong>Health</strong>’s Action<br />
The provider <strong>of</strong> New Zealand’s telephone triage<br />
system, <strong>Health</strong>line, is a partnership <strong>of</strong> High<br />
Per<strong>for</strong>mance <strong>Health</strong>care (HPH) and Access <strong>Health</strong>.<br />
St John’s Ambulance is also part <strong>of</strong> the group. HPH<br />
is based in Australia and Access <strong>Health</strong> provides<br />
nurse telephone triage services as part <strong>of</strong> NHS<br />
Direct in England. Between them they have<br />
substantial experience at providing this kind <strong>of</strong><br />
service.<br />
<strong>Health</strong>line will provide a telephone triage service<br />
to 650,000 people in four identified pilot areas<br />
(Northland, Gisborne/East Cape, Canterbury and<br />
West Coast/Buller).<br />
Pharmacy: Needs to Adapt<br />
Issues<br />
The current regulatory environment is outdated.<br />
Pharmacists no longer produce medicines and are<br />
largely reduced to dispensing pre-packaged<br />
product. The current system is costly <strong>for</strong> both<br />
pharmacists and us. Pharmacists are strongly<br />
unionised by the Pharmacy Guild, which continues to<br />
promote the small business owner aspect <strong>of</strong> pharmacy.<br />
22
Contracts are currently provider-focused with poor<br />
links to health gain. The technical skills <strong>of</strong><br />
pharmacists are under-utilised.<br />
Personal <strong>Health</strong>’s Action<br />
• We have significantly cleared the backlog <strong>of</strong><br />
contractual issues, including settlement <strong>of</strong><br />
outstanding maximum dispensing queries and<br />
the southern pharmacy contract price pool<br />
reviews <strong>for</strong> 1998/99, 1999/2000 and 2000/01.<br />
• We have driven improvements in HBL payment<br />
processes, and are close to implementing<br />
electronic claiming.<br />
• We are working with the sector to identify roles<br />
<strong>for</strong> pharmacy to make use <strong>of</strong> their clinical skills<br />
in patient medicine management.<br />
• We have linked development <strong>of</strong> a pharmacy<br />
strategy with developments in integrated care<br />
and primary care strategies.<br />
Laboratory Contracts: Poised to<br />
Move Forward<br />
Issues<br />
The HFA has consulted on strategies aimed at<br />
managing expenditure on laboratory tests. The<br />
reasons <strong>for</strong> wanting to introduce change include:<br />
• Lack <strong>of</strong> evidence that prices are at the correct<br />
level and some evidence that they are too high.<br />
• Lack <strong>of</strong> competition in the community<br />
laboratory sector over price. Sonic <strong>Health</strong>care,<br />
an Australian company, now owns 65-70<br />
percent <strong>of</strong> the New Zealand community<br />
laboratory sector.<br />
• Regional discrepancies in availability <strong>of</strong> tests<br />
and standard contract terms and conditions,<br />
including quality requirements.<br />
• Increasing utilisation at a higher level than the<br />
increase in health funding. Expenditure has<br />
increased from $116 million (1993/94) to<br />
$172.5 million (99/00).<br />
• A desire by hospital laboratories to enter the<br />
community laboratory business.<br />
Developing a strategy has not been easy. None <strong>of</strong><br />
the RHAs managed. We have, and we are poised to<br />
implement it.<br />
Personal <strong>Health</strong>’s Action<br />
• Developed and implementing strategies to<br />
manage demand, driven by contracting with<br />
primary care organisations and tendering <strong>for</strong><br />
supply <strong>of</strong> a best practice advisory service.<br />
• Consultation on comprehensive supply side<br />
strategies is complete and is waiting on the new<br />
Government be<strong>for</strong>e proceeding. As part <strong>of</strong> that<br />
strategy, we are working towards opening the<br />
market to competition from HHS laboratories.<br />
• There is no single answer - each case will need<br />
a tailored solution.<br />
Maternity: Direction Correct but<br />
Improvements Required<br />
The National <strong>Health</strong> Committee’s maternity<br />
services review this year aimed ‘to consolidate,<br />
refine and render consistent what is already a<br />
workable and potentially equitable structure’.<br />
The recommendations made by the NHC did not<br />
reverse the existing maternity framework.<br />
Issues<br />
The major issue is poor relationships between<br />
providers. Access is also an issue - some women<br />
have difficulty accessing unbiased in<strong>for</strong>mation on<br />
maternity services. Emergency specialist services<br />
<strong>for</strong> women in rural areas also need to be addressed.<br />
The HFA has concerns about poor per<strong>for</strong>mance by<br />
some Leader Maternity Careers (LMC) and some<br />
hospitals.<br />
Personal <strong>Health</strong>’s Action<br />
• We are exploring the development <strong>of</strong> regional<br />
primary maternity networks to provide<br />
in<strong>for</strong>mation to patients and manage<br />
relationships with other providers.<br />
• We are finalising referral guidelines <strong>for</strong> specialist<br />
services<br />
• We have established a maternity ‘Roadside to<br />
Bedside’ focus group, and are addressing<br />
emergency services <strong>for</strong> rural women<br />
• We are finalising a comprehensive audit<br />
programme that complements the LMC audit<br />
programme and the cultural audit currently<br />
being conducted on all hospitals.<br />
HFA Improving Our <strong>Health</strong> 23
Accident Insurance Re<strong>for</strong>m:<br />
Significant Risks<br />
Issues<br />
The Accident Insurance Act has required us to<br />
identify costs to insurers <strong>of</strong> accident services.<br />
The re<strong>for</strong>m has several significant risks, all <strong>of</strong> which<br />
get carried by Personal <strong>Health</strong>:<br />
• Risks <strong>of</strong> providers shifting accident costs from<br />
ACC to the HFA due to higher compliance costs<br />
associated with lodging claims with ACC.<br />
• Comparability <strong>of</strong> the levy paid by ACC ($221<br />
million, 1999/00) and the actual costs <strong>of</strong><br />
delivering accident-related public health acute<br />
services.<br />
• Poor quality <strong>of</strong> in<strong>for</strong>mation collected and<br />
managed by hospitals to in<strong>for</strong>m the purchase<br />
<strong>of</strong> accident related services.<br />
We endorse the direct purchase by an accident<br />
insurer <strong>of</strong> primary based services, except <strong>for</strong><br />
pharmacy and laboratory. The Crown currently<br />
has exemption under the Commerce Act <strong>for</strong> fixing<br />
pharmaceutical and laboratory prices. The Crown<br />
gains negotiating leverage by including those<br />
volumes related to accidents.<br />
Future options <strong>for</strong> funding accident-related<br />
treatment must take into account the following<br />
issues:<br />
• Transaction costs <strong>for</strong> providers and funders<br />
increase in direct relation to the number <strong>of</strong><br />
purchasers and purchasing frameworks.<br />
• Hospital in<strong>for</strong>mation management systems are<br />
in transition from bulk purchasing (which did<br />
not require detailed in<strong>for</strong>mation on the tracking<br />
<strong>of</strong> individual patient costs). Changes putting<br />
pressure on hospital in<strong>for</strong>mation systems must<br />
be managed with the sector, giving clear signals<br />
on in<strong>for</strong>mation needs.<br />
• The public is confused about their entitlements,<br />
particularly the variation between accidents and<br />
illnesses. Changes varying the criteria and<br />
access to publicly funded services must be<br />
clearly communicated.<br />
Personal <strong>Health</strong>’s Action<br />
We are working to improve the tagging <strong>of</strong> accidentrelated<br />
scripts and tests to ensure in<strong>for</strong>mation on<br />
actual volumes is improved. Another priority is<br />
improving the transparency <strong>of</strong> in<strong>for</strong>mation on the<br />
cost/volumes <strong>of</strong> accident-related treatment to<br />
enable in<strong>for</strong>med decision making on future funding<br />
<strong>of</strong> acute accident treatment.<br />
We are improving the in<strong>for</strong>mation on accident<br />
volumes/costs <strong>for</strong> the calculation <strong>of</strong> the public<br />
health acute services levy through:<br />
• Surveying compliance costs to assess the<br />
additional compliance costs imposed on<br />
hospitals and assessing funding options.<br />
• Monthly communication with hospitals to<br />
ensure in<strong>for</strong>mation in implementing the new<br />
regime.<br />
• Analysis <strong>of</strong> hospitals’ routine reporting to<br />
calculate the Public <strong>Health</strong> Acute Services Levy<br />
<strong>for</strong> 2000/01.<br />
Quality: Trans<strong>for</strong>ming the Sector<br />
Issue<br />
A focus on the quality <strong>of</strong> provision <strong>of</strong> health services<br />
has become a feature <strong>of</strong> health systems<br />
internationally. A culture <strong>of</strong> quality and selfimprovement<br />
is rapidly being established.<br />
Some argue that the health sector is the sector<br />
where up-to-date ideas about quality management<br />
have gained least traction. Partly, this is because <strong>of</strong><br />
the sector’s reliance on management by medical<br />
colleges.<br />
There are very major issues in quality improvement.<br />
Those issues include: the setting <strong>of</strong> standards <strong>for</strong><br />
all providers; continuous quality improvement;<br />
provider self-improvement programmes; and<br />
credentialling <strong>of</strong> providers.<br />
The future thinking quality programmes under<br />
development internationally, and being kick-started<br />
in Personal <strong>Health</strong>, are evidence-based health<br />
indicators and monitoring programmes. The belief<br />
is the development <strong>of</strong> these clinical indicator<br />
frameworks will provide territory <strong>for</strong> radical<br />
trans<strong>for</strong>mation <strong>of</strong> clinical services in the future.<br />
Personal <strong>Health</strong>’s Action<br />
Our key objectives during the past year have been:<br />
• Development <strong>of</strong> initiatives to respond to major<br />
quality and safety issues which will arise, with<br />
24
a budget <strong>of</strong> $1.65 million (in addition to the $2<br />
million allocated to investigate Gisborne<br />
pathology services).<br />
• Planning the implementation <strong>of</strong> the <strong>Health</strong> and<br />
Disability Sector Standards.<br />
• Developing evidence-based quality in hospitals.<br />
• Developing quality improvement and<br />
purchasing strategies <strong>for</strong> specific services<br />
(particularly Pharmacies, WellChild, and<br />
Maternity Services).<br />
• Managing the investigation into cervical<br />
screening/laboratory issues in Gisborne.<br />
Sector Standards Being Developed<br />
Issues<br />
These standards will provide <strong>for</strong> assessment <strong>of</strong><br />
providers against a common set <strong>of</strong> safety and quality<br />
requirements. We anticipate the standards will be<br />
a legal requirement, initially applying to services<br />
subject to licensing/regulation requirements<br />
(mainly residential or in-patient/out-patient<br />
hospital services).<br />
Parts <strong>of</strong> the standards have significant short/<br />
medium term cost implications, according to<br />
providers (mainly hospitals). Cost implications are<br />
likely, but there is insufficient in<strong>for</strong>mation available<br />
to enable us to estimate this accurately. Providers<br />
state that the costs are in the tens <strong>of</strong> millions.<br />
Personal <strong>Health</strong>’s Action<br />
Providers have a contractual obligation to use 1999/<br />
2000 as a year <strong>for</strong> planning, in turn we have<br />
developed an evaluation programme. By May 2000<br />
we will have comprehensive national in<strong>for</strong>mation<br />
about the current compliance <strong>of</strong> HHSs and the time/<br />
resources required to achieve compliance.<br />
This in<strong>for</strong>mation will be fed into our sustainable<br />
pricing projects, to ensure the cost <strong>of</strong> quality has<br />
been adequately considered. We anticipate using<br />
this approach to evaluate other providers, including<br />
hospices and Children’s <strong>Health</strong> Camps.<br />
We have been closely involved in the development<br />
<strong>of</strong> the Sector Standards, and will continue to work<br />
with the sector to develop the process <strong>for</strong><br />
credentialling designated agencies, and application<br />
<strong>of</strong> the standards. It is essential these issues are<br />
worked through in close consultation with all<br />
affected parties in order to achieve the standards’<br />
potential. We have arranged <strong>for</strong> a discussion<br />
session with a <strong>Health</strong> and Disability Sector<br />
Standards panel to be on the agenda <strong>of</strong> the Evidence<br />
Based Quality Workshop (see quality improvement<br />
activities in HHSs also).<br />
Evidence Based Quality in HHSs<br />
Issues<br />
Consumer Assurance<br />
Progressing the ability <strong>of</strong> HHSs to listen to the voice<br />
<strong>of</strong> the consumers, using methods including:<br />
• Consumer advisory groups.<br />
• Customer satisfaction surveys.<br />
• Complaints management.<br />
Reducing Errors and Increasing Safety<br />
• Development and improvement <strong>of</strong> healthcare<br />
safety reporting systems.<br />
• Providing <strong>for</strong> timely standardised reporting <strong>of</strong><br />
sentinel and adverse events to in<strong>for</strong>m central<br />
agencies and maintain public confidence.<br />
<strong>Health</strong> and Disability Service Safety Standards<br />
• Compliance by all HHSs completed be<strong>for</strong>e July<br />
2002.<br />
Infection Control<br />
• Improvement in systems that protect patients<br />
and healthcare workers.<br />
<strong>Health</strong>care Work<strong>for</strong>ce<br />
• Work<strong>for</strong>ce planning.<br />
• Retention and recruitment.<br />
• Clinical risk management.<br />
• Credentialling systems.<br />
Quality Oversight<br />
• Making quality explicit - clear aims <strong>for</strong><br />
improvement, improving processes and<br />
eliminating waste.<br />
• Fostering evidence-based practice.<br />
Advancing Quality Measurement<br />
• Standardised measures to track healthcare<br />
progress in clinical outcomes and indicators.<br />
We have undertaken a substantial programme <strong>of</strong><br />
quality improvement activities with HHSs over the<br />
past year, to articulate the quality imperatives <strong>for</strong><br />
HFA Improving Our <strong>Health</strong> 25
medical and surgical secondary/tertiary public<br />
providers, and to initiate projects addressing<br />
national deficits in systems fundamental <strong>for</strong> safe<br />
clinical care.<br />
We have worked closely with the HHSs and<br />
contracted project teams. Audits have been used<br />
to evaluate the current activity within each HHS<br />
and the results have been drawn together on a<br />
national basis. They are being used <strong>for</strong> further<br />
discussion about quality improvement activities<br />
which can be planned on a national and local basis.<br />
Key projects and achievements include:<br />
• Responding to the Stent Report on Canterbury<br />
<strong>Health</strong>.<br />
• Reviewing the credentialling <strong>of</strong> medical<br />
practitioners.<br />
• Reviewing incident reporting systems.<br />
• Auditing complaints management systems.<br />
• Ongoing audit <strong>of</strong> acute admissions.<br />
• Participating in the review <strong>of</strong> HHS consumer<br />
satisfaction surveys. Further details <strong>of</strong> each<br />
project are given below.<br />
Quality Improvement Activities in Non HHS<br />
Providers<br />
Pharmacy<br />
A comprehensive national pharmacy audit has been<br />
implemented with the introduction <strong>of</strong> new<br />
pharmacy contracts (from October 1998) built on<br />
evolution and education. The aim is <strong>for</strong> continuous<br />
improvement <strong>of</strong> pharmacy services. We want to<br />
contribute to quality improvement, maximise<br />
appropriate claiming <strong>of</strong> the pharmaceutical benefit<br />
and <strong>of</strong>fer support to pharmacies in meeting quality<br />
standards.<br />
Child <strong>Health</strong><br />
We are working jointly with Children’s <strong>Health</strong><br />
Camps (CHC) to evaluate their services against the<br />
<strong>Health</strong> and Disability Sector Standards, and a survey<br />
<strong>of</strong> expectations <strong>of</strong> those who refer children to health<br />
camps. This work will significantly contribute<br />
towards the development <strong>of</strong> a clear strategy <strong>for</strong> the<br />
development <strong>of</strong> services provided by CHC.<br />
It will be completed by March 31, 2000.<br />
In early 2000 we will be evaluating (with providers)<br />
the effectiveness <strong>of</strong> the new money allocated to<br />
WellChild services earlier this year. This will<br />
complement the development <strong>of</strong> national standards<br />
and specifications, which will be supported by a<br />
comprehensive review <strong>of</strong> the services currently<br />
provided by WellChild providers.<br />
Maternity<br />
An audit <strong>of</strong> the cultural appropriateness <strong>of</strong><br />
maternity facilities <strong>for</strong> Maori is underway.<br />
This issue was raised by our consumer satisfaction<br />
survey (completed mid 1999) and the survey<br />
carried with the NHC review. It is due to report in<br />
April 2000.<br />
Youth <strong>Health</strong><br />
We have completed an audit <strong>of</strong> the One Stop Shops<br />
in the Wellington region <strong>of</strong> the HFA, which will<br />
contribute towards the development <strong>of</strong> improved<br />
contracts and a wider youth health strategy.<br />
There are two key activities to support the<br />
programme:<br />
1. MEDSAFE is auditing community pharmacies<br />
against the criteria <strong>of</strong> the Pharmacy Quality<br />
Audit (PQA). The HFA, MoH and the<br />
Pharmaceutical Society jointly fund these<br />
audits.<br />
2. HBL is monitoring claiming pr<strong>of</strong>iles, pharmacy<br />
feedback reports and on site selected audits.<br />
26
Clinical Issues and What We are Doing<br />
Waiting Times: Patient Focused<br />
Care<br />
Issues<br />
The waiting times project is an innovative and<br />
international first, a project to bring order to one<br />
<strong>of</strong> the grey areas <strong>of</strong> health management.<br />
Historically, decisions about who gets elective<br />
surgery have been poorly prioritised and sometimes<br />
distorted by relying on individual judgement or a<br />
specialist’s power in a hospital. The project puts<br />
nationally consistent systems in place, based on<br />
clinical criteria, to make sure that those who most<br />
need surgery get it first.<br />
Correct ordering <strong>of</strong> priority means that any<br />
additional money that comes into elective surgery<br />
in the health sector does the most good possible.<br />
The principles <strong>of</strong> the project are as follows:<br />
• Patients should know when, where and what<br />
treatment is available to them within a fixed<br />
period <strong>of</strong> time.<br />
• Everyone, regardless <strong>of</strong> location, is entitled to<br />
the same level <strong>of</strong> service to address the same<br />
level <strong>of</strong> need and ability to benefit.<br />
• Timely access to first assessments and services,<br />
and elective services prioritised on a fair,<br />
transparent and consistent basis nation-wide is<br />
required.<br />
There is now significant acceptance <strong>of</strong> the project<br />
by clinicians and providers. Major system<br />
implementation has taken place. Great ef<strong>for</strong>t has<br />
gone into developing nationally consistent criteria.<br />
Draft national clinical priority tools are currently<br />
being circulated.<br />
The waiting times project raises a number <strong>of</strong><br />
important ethical issues about urgency <strong>of</strong> need<br />
versus ability to benefit. In practice, however,<br />
clinicians take a practical view <strong>of</strong> what needs to be<br />
done in developing the clinical priority criteria.<br />
We are in the early phase <strong>of</strong> development so the<br />
monitoring and evaluation aspects are important.<br />
Diagnostics and some follow-up checks are being<br />
devolved to primary care, leaving money and time<br />
<strong>for</strong> hospital clinicians to improve further the<br />
elective surgery situation.<br />
Personal <strong>Health</strong>’s Action<br />
The <strong>for</strong>mation <strong>of</strong> clinical working groups draws<br />
on pr<strong>of</strong>essional and patient groups to develop<br />
nationally consistent prioritisation tools to:<br />
• Score new patient inflows.<br />
• Re-score patients scored under regional tools.<br />
• Adjust local access thresholds to the new<br />
scoring system.<br />
• Progress from regional use <strong>of</strong> tools to national<br />
consistency.<br />
Our progress has been faster than anticipated <strong>for</strong><br />
the implementation <strong>of</strong> the clinical criteria.<br />
There has been a substantial commitment from the<br />
medical community to development <strong>of</strong> these tools.<br />
We have developed a robust strategy to measure<br />
waiting list outcomes, using booking system data<br />
to ensure alignment with hospital need and capacity<br />
issues, determining more accurate financially<br />
sustainable thresholds by hospitals.<br />
In addition, provision <strong>of</strong> audit and monitoring<br />
processes will ensure quality improvement in<br />
hospital data collection systems.<br />
The system is not fully developed. We are now able<br />
to look up and down the country to identify the<br />
hot spots. We still do not fully understand the<br />
patient flows enough to give a firm view on the<br />
gap between what we currently are able to purchase<br />
(the financially sustainable threshold) and what we<br />
would like to purchase (the clinically sustainable<br />
threshold).<br />
HFA Improving Our <strong>Health</strong> 27
Progress to Date<br />
Patients Waiting <strong>for</strong> Surgery<br />
Number <strong>of</strong> patients on inpatient waiting lists<br />
The number <strong>of</strong> patients waiting <strong>for</strong><br />
surgery has decreased. This is due to<br />
accurate data collection and active<br />
management <strong>of</strong> the patients between the<br />
primary and secondary sectors.<br />
100,000<br />
80,000<br />
60,000<br />
40,000<br />
20,000<br />
0<br />
Jun 96 Jun 97 Dec 98 Mar 99 Jun 99<br />
Year<br />
Jun 96<br />
Jun 97<br />
Dec98<br />
Mar 99<br />
Jun 99<br />
Patients Waiting <strong>for</strong> Surgery<br />
89,620<br />
79,897<br />
68,625<br />
60,929<br />
50,422<br />
60,000<br />
Patients Waiting <strong>for</strong> First Specialist Assessment<br />
Total patients waiting >6 months<br />
The number <strong>of</strong> people waiting more<br />
than six months <strong>for</strong> a first specialist<br />
assessment has decreased, due to first<br />
specialist assessment management<br />
processes and care and review strategies<br />
being developed and implemented<br />
throughout the country.<br />
50,000<br />
40,000<br />
30,000<br />
20,000<br />
10,000<br />
0<br />
1st Quarter<br />
2nd Quarter 3rd Quarter 4th Quarter<br />
Year 98/99<br />
1st Quarter<br />
2nd Quarter<br />
3rd Quarter<br />
4th Quarter<br />
Patients Waiting <strong>for</strong> Assessment<br />
47,729<br />
45,468<br />
45,372<br />
35,774<br />
28
Complex Medicine: Managing the<br />
Issue<br />
Issues<br />
We have developed national referral protocols and<br />
business rules to define policy, eligibility and access<br />
criteria <strong>for</strong> complex (<strong>of</strong>ten high pr<strong>of</strong>ile) situations<br />
involving special high cost treatments, exceptional<br />
circumstances <strong>for</strong> patients, or where patients have<br />
to be transferred to a different region.<br />
To date, a national case manager has been put in<br />
place to oversee these services. Systems, such as a<br />
database <strong>of</strong> cases and more robust approval<br />
procedures, are being developed.<br />
Special High Cost Treatments<br />
We fund special high cost patient treatments with<br />
a budget <strong>of</strong> $14.7 million, covering:<br />
• Medical treatment overseas.<br />
• Simultaneous pancreas and kidney transplants.<br />
• Treatment by private providers.<br />
• New technologies/treatments.<br />
• Tolerisation.<br />
• Hospital high cost treatment items not included<br />
in base contracts, <strong>for</strong> example, heart/lung<br />
transplants.<br />
• Liver treatments.<br />
• Complex patient transfers between regions.<br />
Exceptional Circumstances<br />
We provide <strong>for</strong> financial assistance <strong>for</strong> eligible<br />
persons who require pharmaceuticals, but whose<br />
needs cannot be met under PHARMAC’s<br />
Pharmaceutical Schedule. Approximately $850,000<br />
is allocated annually.<br />
Inter-regional Flows<br />
The budget <strong>for</strong> patient transfers between regions<br />
is $75 million annually. The new protocol<br />
developed by the HFA covers:<br />
• Acute and arranged admissions to a public<br />
hospital which is outside a patient’s region<br />
• Elective, acute and arranged admissions <strong>of</strong><br />
persons who are referred from a hospital which<br />
is outside their region.<br />
Personal <strong>Health</strong> intends devolving patient transfers<br />
to hospital contracts and this is already happening.<br />
This area <strong>of</strong> public sector healthcare requires<br />
ongoing development and solutions related to:<br />
• Transport and accommodation approvals and<br />
payments associated with patient transfers.<br />
• Review <strong>of</strong> the process <strong>for</strong> examining exceptional<br />
circumstances applications.<br />
• Clarity around the cost utility analysis process<br />
with the move to evidence-based medicine<br />
Personal <strong>Health</strong> will conduct a review <strong>of</strong> these<br />
arrangements this year.<br />
Diabetes: Moving Forward<br />
Issues<br />
Diabetes is a Maori health priority and a priority<br />
<strong>for</strong> disease state management.<br />
There are about 120,000 people with diabetes, with<br />
potentially a further 40,000 - 60,000 undiagnosed.<br />
The rate is increasing by 3 percent annually.<br />
Maori and Pacific Islands people have a nearly three<br />
times higher prevalence, and their diabetes<br />
mortality rate in the 40-65 year age range is nearly<br />
10 times higher than <strong>for</strong> other New Zealanders.<br />
In some areas 50 percent <strong>of</strong> renal failure is caused<br />
by diabetes and last year there were 548 lower limb<br />
amputations in people with diabetes. This is<br />
unacceptably high. Admissions to hospitals with<br />
diabetes as the major diagnosis cost $19 million<br />
(1998/99) but when hospitalisation <strong>for</strong><br />
complications and other healthcare services are<br />
included, the total health cost has been estimated<br />
at $200-250 million annually.<br />
There is regional variation in education and some<br />
treatment services. Nationally, only 30 percent <strong>of</strong> the<br />
necessary eye screening (to reduce blindness in<br />
people with diabetes) is being funded. Early detection<br />
<strong>of</strong> diabetes is important and needs careful planning.<br />
The core <strong>of</strong> our strategy is to introduce in<strong>for</strong>mationbased<br />
disease management techniques.<br />
These techniques allow providers to look across<br />
traditional boundaries and manage patients far<br />
more effectively. The strategy is moving in tandem<br />
with the primary care strategy in particular.<br />
Implementation <strong>of</strong> our diabetes strategy is well<br />
under way.<br />
HFA Improving Our <strong>Health</strong> 29
Personal <strong>Health</strong>’s Action<br />
• Increased diabetes funding by $5 million<br />
annually per year (from 1999). There is<br />
justification <strong>for</strong> similar increases in funding<br />
next year.<br />
• Reduction <strong>of</strong> barriers (cost, access, and cultural)<br />
to high quality routine care <strong>for</strong> those at highest<br />
risk (Maori, Pacific Islands people and low<br />
socio-economic groups).<br />
• Building strong feedback links with patient<br />
organisations.<br />
• Developing guidelines <strong>for</strong> diabetes services and<br />
a clinical indicators framework to monitor<br />
per<strong>for</strong>mance. The national diabetes working<br />
group <strong>of</strong> clinicians and consumers is already<br />
established.<br />
• Commitment to involve patients and clinicians<br />
in teams (regional or locality level) in<br />
monitoring diabetes services in their areas and<br />
recommending improvements. Terms <strong>of</strong><br />
reference have been developed, and<br />
consultation is now occurring.<br />
• Integration <strong>of</strong> education into primary care<br />
treatment, with specific choices <strong>for</strong> Maori and<br />
Pacific Islands people (extra funding has been<br />
allocated).<br />
• Progressively increasing the funding <strong>for</strong> allied<br />
diabetes services in primary care (nurse<br />
educators, dieticians, and podiatrists) and Maori<br />
and Pacific Islands provider organisations<br />
prepared to maintain active diabetes registers<br />
and present their data to regional/locality<br />
diabetes teams.<br />
• Negotiations with primary care organisations<br />
<strong>for</strong> an annual review and individual treatment<br />
plan <strong>for</strong> every person with diabetes, with the<br />
aim to make this service free (at least) to<br />
Community Service Cardholders. This review<br />
will be used to detect complications early, and<br />
update the diabetes register used to monitor<br />
diabetes in the enrolled population.<br />
• A planned increase in funding <strong>for</strong> mobile<br />
services, eye screening 2000, and monitoring<br />
<strong>of</strong> increased access using in<strong>for</strong>mation from the<br />
diabetes registers.<br />
• Development <strong>of</strong> proposals <strong>for</strong> early screening,<br />
targeted at high-risk groups.<br />
Asthma: A High Priority<br />
Issues<br />
More than 500,000 New Zealanders have asthma<br />
and the figure is growing inexplicably. The number<br />
hospitalised is increasing despite advances in<br />
therapy, asthma treatment plans and the good<br />
supply <strong>of</strong> new medications and devices.<br />
There is a high incidence amongst Maori and Pacific<br />
Islands peoples. Increasing hospital admissions are<br />
partially explained by Maori and Pacific Islands<br />
peoples’ poor access to care and the use <strong>of</strong> hospital<br />
emergency departments by people who should have<br />
seen their primary care provider earlier.<br />
Other contributory factors include patients’ failure<br />
to use drugs and devices appropriately, and lack <strong>of</strong><br />
monitored care programmes.<br />
Asthma is the second <strong>of</strong> our disease state<br />
management programmes.<br />
Personal <strong>Health</strong>’s Action<br />
• $2.7 million <strong>for</strong> a disease management strategy,<br />
including $400,000 to help develop Maori<br />
provider skills. Contracts with providers <strong>for</strong><br />
provision <strong>of</strong> additional services should be<br />
signed next February.<br />
• Formation <strong>of</strong> a national asthma working group<br />
drawing on pr<strong>of</strong>essionals and patient groups to<br />
provide advice.<br />
• Development <strong>of</strong> quality and service<br />
per<strong>for</strong>mance monitoring.<br />
• Liaison with PHARMAC about the appropriate<br />
use <strong>of</strong> drugs and with the Asthma and<br />
Respiratory Foundation <strong>for</strong> the possible funding<br />
<strong>of</strong> some foundation projects.<br />
Heart Disease: Preparing the Way<br />
Issues<br />
Coronary artery disease remains one <strong>of</strong> the major<br />
causes <strong>of</strong> mortality, particularly among<br />
males. Maori men have a particularly high<br />
mortality rate, which is 1.7 times higher than<br />
other males. Maori women have a mortality rate<br />
30
at nearly twice that <strong>of</strong> non-Maori and equivalent<br />
to New Zealand males.<br />
Coronary artery disease can be treated by drugs,<br />
angioplasty (PTCA) and/or coronary artery by-pass<br />
surgery (CABG), depending on the stage <strong>of</strong> the<br />
disease. Treatment <strong>for</strong> coronary artery disease spans<br />
the primary, secondary and tertiary sectors.<br />
There are a number <strong>of</strong> problems in the provision<br />
<strong>of</strong> cardiac services. A review <strong>of</strong> cardiac services<br />
carried out in late 1998 identified:<br />
• Maori had the lowest intervention rates <strong>for</strong><br />
CABG yet Maori have the highest mortality rates<br />
from coronary artery disease.<br />
• Regional variations in waiting lists <strong>for</strong> PTCA<br />
and CABG. Canterbury <strong>Health</strong> had the largest<br />
waiting list <strong>for</strong> PTCA and Capital Coast <strong>Health</strong><br />
had the highest waiting list <strong>for</strong> CABG.<br />
• Variation in the public/private intervention rates<br />
<strong>for</strong> both PTCA and CABG which has a regional<br />
impact.<br />
• Cardiology and cardiac surgery services are<br />
inefficiently purchased, mainly separately,<br />
which can lead to inefficiencies in the delivery<br />
<strong>of</strong> cardiac services.<br />
There is fragmentation <strong>of</strong> primary and secondary<br />
care, a lack <strong>of</strong> quality primary care service and a<br />
lack <strong>of</strong> emphasis on rehabilitation. Again, we are<br />
proposing an up-to-date disease state management<br />
approach to management <strong>of</strong> heart disease. The issue<br />
is identified but not actioned. It is third on the<br />
priority list after diabetes and asthma.<br />
Personal <strong>Health</strong>’s Action<br />
• Establish capacity to undertake work.<br />
• Look at promotion <strong>of</strong> pharmaceutical<br />
interventions which reduce hospital admission<br />
and need <strong>for</strong> surgery.<br />
• Implement quality standards with primary care<br />
to ensure patients at risk are given maximum<br />
chance to maintain their health.<br />
Oral <strong>Health</strong>: Focus on Youth<br />
Issues<br />
Oral health services have become progressively out<br />
<strong>of</strong> kilter with changes in society. There have been<br />
few major changes over the last 50 years and they<br />
have become progressively dysfunctional.<br />
In particular, oral health services have failed to<br />
adapt to the growing needs <strong>of</strong> adolescents and<br />
Maori. There are long standing issues around adult<br />
Maori oral health and variations in outpatient and<br />
inpatient services provided by hospitals.<br />
Personal <strong>Health</strong> has seized the opportunity created<br />
by concern about inadequate payment <strong>of</strong> dentists<br />
as an opportunity to review oral health services<br />
from the ground up. This has been very well<br />
received by the sector and has revealed a strong<br />
public health ethos and enthusiasm <strong>for</strong> change in<br />
providers. We have engaged the sector through a<br />
joint working party (a Technical Advisory Group)<br />
with representatives from providers, sector<br />
organisations, the Maori <strong>Health</strong> Commission, and<br />
pr<strong>of</strong>essional bodies. This joint working party has<br />
been highly effective at working through the issues<br />
facing oral health services.<br />
The Personal <strong>Health</strong> initiative has been driven by<br />
a need to reverse the decline in oral health. We<br />
also have a strong desire to link oral health back<br />
into the mainstream <strong>of</strong> health care. An example <strong>of</strong><br />
mainstreaming is a recent initiative to contract with<br />
oral health Well Child providers to educate other<br />
Primary care providers on the importance <strong>of</strong> oral<br />
health. A strategy has been developed in<br />
conjunction with the <strong>Ministry</strong> <strong>of</strong> <strong>Health</strong> and awaits<br />
approval. The strategy identifies the need <strong>for</strong><br />
sustainable funding <strong>for</strong> dentists and opportunities<br />
<strong>for</strong> dental therapists if deregulation occurs.<br />
The <strong>Ministry</strong> <strong>of</strong> Education wants to transfer<br />
purchasing responsibility <strong>for</strong> school dental clinics<br />
to the health vote. There are currently<br />
inconsistencies between the HFA and WINZ<br />
methods <strong>for</strong> funding low-income adult dental care,<br />
resulting in confusion <strong>for</strong> providers and consumers.<br />
Personal <strong>Health</strong>’s Action<br />
• Developing more appropriate services,<br />
especially educational methods and<br />
preventative services <strong>for</strong> Maori.<br />
Existing successful services <strong>for</strong> Maori will be<br />
encouraged and duplicated.<br />
• Publicly consulting on options <strong>for</strong> service<br />
provision to encourage teenagers and children<br />
to access services.<br />
HFA Improving Our <strong>Health</strong> 31
• Inviting technical advisory groups to contribute<br />
in assessing reporting requirements and pricing<br />
methods <strong>for</strong> child and adolescent services<br />
• Developing capitated contracting methods,<br />
allowing clinical freedom and encouraging<br />
preventative management.<br />
• Encouraging service integration and focusing<br />
on prevention and education.<br />
• Supporting the <strong>for</strong>mation <strong>of</strong> whanau-based<br />
services <strong>for</strong> Maori.<br />
• Continuing to support the deregulation <strong>of</strong><br />
dental therapists and the Oral <strong>Health</strong> Forum<br />
2000.<br />
The HFA is utilising current budgets <strong>for</strong> hospital<br />
dental services more effectively and working with<br />
the sector to identify additional in<strong>for</strong>mation<br />
required.<br />
Immunisation: Revamp in Action<br />
Issues<br />
Immunisation coverage has improved but remains<br />
inadequate to prevent cyclical problems such as the<br />
current whooping cough epidemic. Some children<br />
(particularly Maori and Pacific Island) do not have<br />
regular GPs so miss out on immunisation.<br />
Most GPs achieve high coverage rates <strong>for</strong> their<br />
regular child patients. The NHC report reiterated<br />
many <strong>of</strong> the known problems. The HFA has<br />
programmes in place or under development to<br />
address the major recommendations. The agreed<br />
overall target is 95 percent.<br />
The additional cost <strong>of</strong> achieving targets is probably<br />
$10-$15 million annually (excluding catch-up<br />
programmes). Personal <strong>Health</strong> is unlikely to<br />
achieve Funding Agreement targets without<br />
additional resources.<br />
Personal <strong>Health</strong>’s Action<br />
Immunisation strategies in place or being<br />
developed include:<br />
• A comprehensive upgrade <strong>of</strong> the programme<br />
such as opportunistic out-reach immunisation,<br />
and targeting <strong>of</strong> areas <strong>of</strong> poor immunisation<br />
rates, such as South Auckland.<br />
• Primary care initiatives in Rotorua, Union<br />
<strong>Health</strong> Services and elsewhere have more than<br />
90 percent coverage. The new primary care and<br />
section 51 initiatives will encourage others to<br />
achieve these results.<br />
• Immunisation promotion through HHS public<br />
health, Well Child, and Maori and Pacific Island<br />
health services. Immunisation co-ordination<br />
will be expanded in 2000. Maori health<br />
initiatives have achieved high coverage, but do<br />
not reach all Maori children.<br />
• Development <strong>of</strong> the Child <strong>Health</strong> In<strong>for</strong>mation<br />
Strategy (e.g. KidZNet in Waikato-Bay <strong>of</strong><br />
Plenty). Electronic reporting will improve<br />
in<strong>for</strong>mation from 2000 and assist programmes<br />
<strong>for</strong> low coverage areas.<br />
Hepatitis B: Screening Introduced<br />
Issues<br />
Hepatitis B is a highly infectious virus, spread by<br />
the exchange <strong>of</strong> body fluids and blood.<br />
Acute infection is unnoticed <strong>for</strong> 90 percent <strong>of</strong><br />
patients, while 10 percent develop jaundice.<br />
Some 10 percent <strong>of</strong> patients develop chronic<br />
infection potentially resulting in liver problems:<br />
cancer and permanent liver damage.<br />
Some 90 percent <strong>of</strong> infants born to a Hepatitis B<br />
positive mother will become chronic carriers.<br />
Some 0.5 percent - 5 percent <strong>of</strong> people infected in<br />
adult life will become carriers. Although the<br />
majority <strong>of</strong> carriers may not suffer adverse<br />
consequences, up to 40 percent may develop<br />
cirrhosis or hepatocellular carcinoma.<br />
The regional distribution <strong>of</strong> infection is highly<br />
variable, predominantly in the North Island.<br />
There are marked ethnic differentials, with the<br />
Maori carrier rate 10 times higher than Europeans.<br />
The Pacific Islands carrier rate is eight times higher<br />
than the European rate and the Asian carrier rate<br />
is similarly high.<br />
Safe and effective vaccines have been available <strong>for</strong><br />
at least a decade but the initial price and lack <strong>of</strong><br />
awareness about Hepatitis B has limited their use.<br />
However, there is a new gull programme <strong>of</strong><br />
immunisation. Vaccination is the mainstay<br />
internationally, but New Zealand is also<br />
implementing a screening programme.<br />
Personal <strong>Health</strong>’s Action<br />
• Approximately $32 million over three years to<br />
fund a Hepatitis B screening programme <strong>for</strong><br />
32
high risk populations in a limited geographic<br />
area; $22 million <strong>for</strong> screening and surveillance;<br />
$10 million <strong>for</strong> secondary/tertiary care.<br />
• Introduced contracts with providers to focus<br />
on 70 percent uptake by the target population<br />
in the North Island over three years: Maori,<br />
Pacific Island and Asian people over 15 years<br />
(an estimated 495,000 people).<br />
• Introduced <strong>for</strong>mal evaluation <strong>of</strong> the programme<br />
over three years, comparing the two models <strong>of</strong><br />
service delivery: Lower North (Hepatitis<br />
Foundation) is community-based, Upper North<br />
(A+ Consortium) is provider-based.<br />
• Development <strong>of</strong> an independent steering<br />
committee to oversee the Hepatitis B<br />
programme.<br />
Sexual and Reproductive<br />
Services: Under the Microscope<br />
Issues<br />
Sexually transmitted diseases are spreading,<br />
particularly among young people and there is a very<br />
high incidence <strong>of</strong> chlamydia.<br />
A number <strong>of</strong> issues have arisen, including<br />
availability <strong>of</strong> specialist services, interaction<br />
between specialist and primary services, funding,<br />
work<strong>for</strong>ce availability and development, and<br />
resources <strong>for</strong> health promotion.<br />
We are particularly pleased with the new sexual<br />
health service in Wellington. We may look to<br />
extend the ideas from this service through the<br />
country, although a full evaluation will need to be<br />
completed.<br />
Personal <strong>Health</strong>’s Action<br />
• We have undertaken a stock take <strong>of</strong> sexual<br />
health service funding and the assessment <strong>of</strong><br />
sexual health services is a priority <strong>for</strong> 2000.<br />
• Increased funding <strong>for</strong> contraception was made<br />
available in 1996/97 and this has been<br />
continued.<br />
Oncology: Reviewing Drugs and<br />
Radiation<br />
Oncology is an area <strong>of</strong> rapid growth and<br />
opportunity to improve care. An ageing population<br />
and new technology mean greater demand <strong>for</strong><br />
resources. The challenge is to make sure resources<br />
are available to the areas <strong>of</strong> greatest benefit.<br />
As with cardiology, there is potential <strong>for</strong> reducing<br />
illness by suitable prevention activities such as<br />
reducing smoking.<br />
Issues<br />
• Capital expenditure on equipment.<br />
• Staffing recruitment and retention in radiation<br />
and oncology.<br />
• Increasing incidence <strong>of</strong> cancer.<br />
• The method <strong>of</strong> assessing new drugs and their<br />
funding.<br />
Personal <strong>Health</strong>’s Action<br />
• Following a waiting time problem in<br />
MidCentral <strong>Health</strong> in May 1999, a working<br />
party was set up with MoH to identify issues<br />
and find solutions. The working party<br />
comprised radiation oncologists, medical<br />
radiation technologists and medical physicists.<br />
Personal <strong>Health</strong> identified the costs <strong>of</strong> providing<br />
radiation oncology, developing methods that<br />
can be used in other sectors.<br />
• This resulted in an effective working<br />
relationship between all participants (including<br />
the working party, HFA, MoH, CCMAU and<br />
hospitals). This will assist in the progress <strong>of</strong><br />
future service review work. The work<br />
completed so far has increased clarity <strong>of</strong> current<br />
costs and sustainable prices, which links with<br />
broader service strategy work on sustainable<br />
pricing and capital investment policy.<br />
• A medical oncology group, similar to the<br />
radiation oncology group, has been recently<br />
<strong>for</strong>med. This group will work with the HFA and<br />
MoH to address some <strong>of</strong> the issues <strong>of</strong> assessment<br />
<strong>of</strong> new treatments.<br />
• Pilot programmes <strong>for</strong> sexual and reproductive<br />
health promotion <strong>for</strong> Pacific Island people were<br />
established in 1997/98 and have now been<br />
evaluated.<br />
HFA Improving Our <strong>Health</strong> 33
Palliative Care: Studied <strong>for</strong> the<br />
First Time<br />
Hospices have been largely funded privately since<br />
they were established in the 1970s. In recent years<br />
some funding has come from Government as<br />
hospices increasingly compete with charities <strong>for</strong><br />
funds. At the same time, the number <strong>of</strong> hospital<br />
and GP referrals to hospices is rising. Hospice New<br />
Zealand believes hospices should be recognised as<br />
a core health area and funded accordingly.<br />
Issues<br />
• Inconsistent access and quality <strong>of</strong> hospice<br />
services nationally.<br />
• Only a small proportion <strong>of</strong> eligible people<br />
receive the complete service.<br />
• Service co-ordination issues between providers,<br />
including fragmentation and duplication.<br />
• Regional differences in funding.<br />
Personal <strong>Health</strong>’s Action<br />
We undertook interim work this year, be<strong>for</strong>e a<br />
national strategy is developed, to assist the most<br />
poorly-funded hospices unlikely to survive financially.<br />
The palliative care strategy is being undertaken<br />
jointly by the HFA, MoH, and NHC. It builds on<br />
the interim (and incomplete) work started by the<br />
NHC two years ago. The team is working with an<br />
advisory group comprising experts and a consumer<br />
representative. A reference group <strong>of</strong> interested<br />
organisations has also been <strong>for</strong>med which will<br />
advise on issues such as child palliative care and<br />
first level consultation.<br />
The following work has been, or is close to being,<br />
completed:<br />
• Definition, principles and a model <strong>of</strong><br />
palliative care.<br />
• Stocktaking <strong>of</strong> contracts <strong>of</strong> all palliative<br />
care providers.<br />
• Analysis <strong>of</strong> questionnaires sent to hospices on<br />
the provision and costs <strong>of</strong> care.<br />
• Analysis <strong>for</strong> determining the need <strong>for</strong><br />
palliative care.<br />
Cervical Screening Investigation:<br />
Gisborne<br />
Issues<br />
In March 1999 the HFA became aware <strong>of</strong> the<br />
per<strong>for</strong>mance <strong>of</strong> Gisborne pathologist Dr Michael<br />
Bottrill, who retired in 1996. An expert advisory<br />
group was established in May which confirmed the<br />
investigation should focus on the initial concern -<br />
Dr Bottrill’s reading <strong>of</strong> cervical smear slides.<br />
Personal <strong>Health</strong>’s action<br />
Twenty-three thousand cervical smear slides (all<br />
from Dr Bottrill’s laboratory between 1991 - 1996)<br />
were re-read last year by a Sydney laboratory. The<br />
investigation affected just over 12,000 women who<br />
had smears read by Dr Bottrill’s laboratory during<br />
this period. In March 2000, following the<br />
completion <strong>of</strong> the re-reading, and subsequent result<br />
matching, all affected women were sent a letter<br />
detailing their individual slide results.<br />
During its investigation, the HFA introduced an<br />
additional range <strong>of</strong> measures to support these<br />
women (both those living in Gisborne and those<br />
now living elsewhere). These measures include:<br />
• Free smears, GP consultations and counselling<br />
services.<br />
• Establishment <strong>of</strong> an 0800 number.<br />
• Facilitation services encouraging women to<br />
access smears.<br />
• Co-ordination services to assist women to<br />
access all public sector entitlements.<br />
• Experienced colposcopy services with<br />
minimum delay <strong>for</strong> women identified with<br />
previously unreported high-grade<br />
abnormalities.<br />
• Special circumstances support, under which the<br />
HFA meets childcare, travel and home support<br />
costs to enable women access to diagnosis and<br />
treatment services.<br />
The total cost <strong>of</strong> the investigation (including the<br />
re-reading and support services) is estimated at $1.5<br />
million. This was budgeted <strong>for</strong> in the 1998/99<br />
financial year and carried <strong>for</strong>ward into the<br />
current one.<br />
34
Throughout the process, the HFA has contacted<br />
women with high-grade abnormalities so that they<br />
can immediately commence treatment. The HFA<br />
sought advice on whether women with previously<br />
unreported low-grade abnormalities should be<br />
contacted during the re-reading. It was advised that<br />
in<strong>for</strong>ming these women at the end <strong>of</strong> the process<br />
did not pose any risk to their health. The HFA made<br />
the necessary services available to deal with these<br />
quickly when result letters were sent out.<br />
Interim results from the first 5,000 slides indicated<br />
substantial under-reporting by Dr Bottrill. This<br />
pattern continued throughout the entire re-reading.<br />
They indicated an extremely high error rate even<br />
allowing <strong>for</strong> potentially increased sensitivity by the<br />
re-reading laboratory. The interim results were<br />
announced publicly because the investigation has<br />
been extended to other work undertaken by Dr<br />
Bottrill.<br />
On the advice <strong>of</strong> the advisory group, the<br />
investigation was initially extended to a re-reading<br />
<strong>of</strong> breast histology specimens. Breast histology is<br />
an area with potential to improve health outcomes<br />
if mis-reading is found and was considered likely<br />
to give the quickest indication whether there is a<br />
pattern <strong>of</strong> mis-reading <strong>of</strong> histology by Dr Bottrill.<br />
The HFA arranged <strong>for</strong> 380 breast histology cases<br />
originally read by Dr Bottrill’s laboratory between<br />
1989 and 1996 to be re-read. A number <strong>of</strong><br />
differences were found and reviewed by an expert<br />
breast surgeon, who determined that these<br />
differences were <strong>of</strong> clinical significance in only two<br />
cases.<br />
Paediatric Specialty Services:<br />
Review Underway<br />
This is a joint project between Personal <strong>Health</strong>,<br />
Paediatric Society <strong>of</strong> New Zealand and MoH.<br />
It ensures nationally consistent access and quality<br />
standards.<br />
• Agreement has been reached <strong>for</strong> a national<br />
paediatric oncology service. Hospitals are now<br />
putting <strong>for</strong>ward plans to meet the agreed quality<br />
guidelines.<br />
• Guidelines <strong>for</strong> Attention Deficit Hyperactivity<br />
Disorder and Downs Syndrome, a national<br />
tumour board and Child <strong>Health</strong> Network are<br />
being developed.<br />
• Joint working groups <strong>of</strong> GPs, nurses, Maori and<br />
Pacific Islands health providers and HFA staff<br />
are looking at pricing <strong>of</strong> primary care services,<br />
definitions <strong>of</strong> the services purchased, future<br />
roles <strong>of</strong> primary care organisations and<br />
in<strong>for</strong>mation requirements and enrolment.<br />
We are analysing the recommendations and cost<br />
<strong>for</strong> all other paediatric subspecialties.<br />
A significant, linked issue is travel and<br />
accommodation policy. Paediatric specialties will<br />
continue to be centralised as quality standards are<br />
implemented. This means more travel <strong>for</strong> patients<br />
and their guardians. A review <strong>of</strong> travel and<br />
accommodation is underway.<br />
It is important to note there is a small margin <strong>of</strong><br />
error associated with all pathology and histology<br />
work. It should also be noted that advances in the<br />
diagnosis <strong>of</strong> breast cancer have helped to reduce<br />
the small chance <strong>of</strong> these errors occurring.<br />
After careful consideration <strong>of</strong> all available<br />
in<strong>for</strong>mation, the Advisory Group has concluded<br />
that the breast histology work by Dr Bottrill’s<br />
laboratory is <strong>of</strong> the standard expected.<br />
The Advisory Group has there<strong>for</strong>e recommended<br />
that the investigation is not extended into any other<br />
areas, and the HFA has accepted this<br />
recommendation.<br />
HFA Improving Our <strong>Health</strong> 35
Personal <strong>Health</strong> —<br />
Financial In<strong>for</strong>mation At A Glance<br />
Personal <strong>Health</strong> Services Budget<br />
Personal <strong>Health</strong> has been responsible <strong>for</strong><br />
managing $3,745.9 billion (67 percent) <strong>of</strong> the<br />
<strong>Health</strong> and Disability Fund ($5.748 billion) <strong>for</strong><br />
public health services provided by the Government<br />
from taxpayer funds.<br />
The following table (sourced from the General<br />
Ledger) provides an overview <strong>of</strong> the services<br />
purchased:<br />
Break-Out <strong>of</strong> the Hospital<br />
Spending<br />
Of the <strong>Health</strong> and Hospital Services (HHSs),<br />
Auckland <strong>Health</strong>care, (an aggregate <strong>of</strong> Auckland<br />
Hospital, Starship, National Women’s and<br />
Greenlane), has by far the largest amount <strong>of</strong> public<br />
money spent on medical surgical services,<br />
at $348 million.<br />
Personal <strong>Health</strong> Services Purchased in 1999/00<br />
Service Grouping<br />
Value $million<br />
Community Services<br />
Child and Youth 73.9<br />
Maternity and Neo-natal 353.4<br />
Oral <strong>Health</strong> 89.2<br />
Pacific People’s <strong>Health</strong> 5.2<br />
General Practice Services 367.4<br />
Population Based Services 42.6<br />
Pharmaceuticals 645.2<br />
Laboratories 172.5<br />
Other Referred Services 47.3<br />
Sub-total 1,806.7<br />
Medical Surgical Services<br />
*Medical surgical 1,968.5<br />
Special High Cost Treatments<br />
and Exceptional Circumstances 14.8<br />
Inter Regional Transfers 55.9<br />
Sub-total 2,039.2<br />
Total 3,745.9<br />
Services purchased.<br />
* Including non-HHS based contracts.<br />
Medical/Surgical Services<br />
expenditure by HHS<br />
Value $million<br />
Auckland <strong>Health</strong>care 348<br />
Waitemata <strong>Health</strong> 87<br />
South Auckland <strong>Health</strong> 172<br />
Northland <strong>Health</strong> 62.5<br />
<strong>Health</strong> Waikato 185.7<br />
Pacific <strong>Health</strong> 81.6<br />
Lakeland <strong>Health</strong> 38.7<br />
Tairawhiti <strong>Health</strong>care 23.7<br />
Taranaki <strong>Health</strong> 47.9<br />
Good <strong>Health</strong> Wanganui 29.1<br />
<strong>Health</strong>care Hawkes Bay 64.9<br />
Midcentral <strong>Health</strong> 79.8<br />
Capital Coast <strong>Health</strong> 154.9<br />
Hutt Valley <strong>Health</strong> 49.2<br />
Wairarapa <strong>Health</strong> 16.8<br />
Nelson Marlborough <strong>Health</strong> 45.1<br />
<strong>Health</strong> South Canterbury 23<br />
Coast <strong>Health</strong> Care 16.5<br />
Canterbury <strong>Health</strong> 234.2<br />
<strong>Health</strong>link South 2.8<br />
<strong>Health</strong>care Otago 96.1<br />
Southern <strong>Health</strong> 37.4<br />
Total 1,898.2<br />
Hospital and <strong>Health</strong> Services spending by 1999/2000<br />
Contract Value, including Waiting Time Fund.<br />
36
Clinical Groupings<br />
Our systems also provide a breakdown <strong>of</strong> service<br />
spending by clinical groupings as set out in the table<br />
below.<br />
Types <strong>of</strong> Admittances<br />
The table below sets out the category <strong>of</strong> hospital<br />
admittances.<br />
Service<br />
Value $million<br />
Admittance Type<br />
Value $million<br />
Cardiology 63.2<br />
Cardiothoracic 58.2<br />
Dermatology 5.0<br />
Ear, Nose and Throat 42.4<br />
Emergency Department 101.6<br />
Endocrinology and Diabetic 13.6<br />
Facility level - Personal <strong>Health</strong> 48.5<br />
Acute 824.7<br />
Elective 350.7<br />
First Specialist 70.4<br />
Follow up 111.0<br />
Outpatient Community 541.4<br />
Total 1,898.2<br />
1999/2000 Contract Value by Admittance Type<br />
Gastroenterology 19.9<br />
General Internal Medical Services 299.9<br />
General Surgery 220.6<br />
Gynaecology 76.8<br />
Haematology 38.2<br />
Infectious Diseases (Venereology) 4.0<br />
Medical Genetics Services 2.0<br />
Medical Surgical - Other 24.3<br />
Neurology 17.5<br />
Neurosurgery 23.8<br />
Oncology 83.9<br />
Ophthalmology 40.7<br />
Orthopaedics 214.8<br />
Paediatric Medical 75.8<br />
Paediatric Medicine 10.7<br />
1999/2000 Paediatric Contract Surgical Value by Service Type 27.8<br />
Palliative Care 2.8<br />
Plastic and Burns 37.7<br />
Renal Medicine 61.0<br />
Respiratory 31.5<br />
Rheumatology 7.8<br />
Spinal Services 3.8<br />
Urology 34.6<br />
Vascular Surgery 19.7<br />
Other 185.8<br />
Total 1,898.2<br />
HFA Improving Our <strong>Health</strong> 37
Indicative Prices and Patient Numbers<br />
Most funding <strong>for</strong> personal health services is spent outside <strong>of</strong> hospitals (55 percent) and paid to private<br />
primary care providers such as GPs and Maori providers. We contract hospitals to provide medical and<br />
surgical services, maternity services and some specific community services.<br />
Here we provide indicative prices <strong>for</strong> the “Top 100” sample <strong>of</strong> elective surgery, ranked in desending order<br />
according to expenditure values.<br />
Top 100 Indicative prices paid by the HFA <strong>for</strong> inpatient hospital<br />
procedures, ranked by total expenditure<br />
Rank<br />
Diagnostic Related Group (DRG) Description<br />
National<br />
Price<br />
1999/00<br />
per patient<br />
Number <strong>of</strong><br />
Discharges<br />
Total<br />
Expenditure<br />
$million<br />
1 Tracheostomy except <strong>for</strong> mouth, larynx or pharynx disorder age >15,<br />
including intensive care and continuous mechnical ventilation $41,027 880 36.1<br />
2 Circulatory disorders with AMI without invasive cardiac investigative<br />
procedure without major complications $ 3,839 5097 19.6<br />
3 Hip replacement without complications $ 8,877 2179 19.3<br />
4 Major small and large bowel procedures with complications $11,516 1654 19.0<br />
5 Trans-vascular percutaneous cardiac intervention $ 7,198 2471 17.8<br />
6 Cerebrovascular disorders except TIA with complications $ 5,758 3076 17.7<br />
7 Respiratory infections or inflammations age >54 with complications $ 4,079 4200 17.1<br />
8 Heart failure and shock $ 2,639 6059 16.0<br />
9 Chronic obstructive airways disease $ 1,919 7368 14.1<br />
10 Coronary bypass without invasive cardiac investigative procedure<br />
without major complications $15,355 801 12.3<br />
11 Hip replacement with complications $10,796 1129 12.2<br />
12 Hip and femur procedures except major joint with complications $ 9,597 1178 11.3<br />
13 Lens procedures without vitrectomy and without complications $ 2,159 4909 10.6<br />
14 Unstable angina with complications $ 2,639 3531 9.3<br />
15 Major small and large bowel procedures without complications $ 7,438 1252 9.3<br />
16 Cardiac pacemaker implantation $12,476 718 9.0<br />
17 Lower extremity and humerus procedures except hip, foot,<br />
femur age
29 Craniotomy with complications $15,115 495 7.5<br />
30 Bronchitis and asthma age 64<br />
or with non-major complications $ 21,353 263 5.6<br />
39 Kidney, ureter and major bladder procedure <strong>for</strong> non-neoplasm $ 5,518 1017 5.6<br />
40 Infections and inflammations <strong>of</strong> bone and joint with miscellaneous<br />
muscular system and connective tissue procedures $ 6,958 802 5.6<br />
41 Tracheostomy <strong>for</strong> multiple significant trauma age >15 $48,944 112 5.5<br />
42 Neonate, admission weight 750-999g $38,867 140 5.4<br />
43 Respiratory neoplasms with complications $ 3,359 1617 5.4<br />
44 Extensive OR procedure unrelated to principal diagnosis $ 5,758 939 5.4<br />
45 Septicaemia age >34 $ 5,038 1071 5.4<br />
46 Abdominal pain or mesenteric adenitis without complications $ 720 7379 5.3<br />
47 Craniotomy without complications $ 8,877 578 5.1<br />
48 Dental extractions and restorations $ 960 5267 5.1<br />
49 Dementia and global disturbances <strong>of</strong> cerebral function $ 5,038 1002 5.0<br />
50 Neonate, admission weight >2499g, without significant OR procedure,<br />
without problem $ 720 6771 4.9<br />
51 Circulatory disorder without AMI with invasive cardiac investigative<br />
procedure without complicating diagnosis and without major<br />
complications $ 1,440 3227 4.6<br />
52 Cellulitis (age >59 without complications) or (age 74 or (age 10-74 with complications) $ 1,440 3117 4.5<br />
55 Circulatory disorder without AMI with invasive cardiac investigative<br />
procedure with complicating diagnosis or with major complications $ 2,399 1864 4.5<br />
56 Neonate, admission weight >2499g, without significant OR procedure,<br />
with major problem $ 2,639 1643 4.3<br />
57 Hand or wrist procedures except major joint $ 1,200 3609 4.3<br />
58 Other OR procedure <strong>for</strong> multiple significant trauma $18,954 220 4.2<br />
59 Major reconstructive vascular procedure without pump with major<br />
complications $14,635 284 4.2<br />
60 S<strong>of</strong>t tissue procedures $ 2,159 1922 4.2<br />
61 Kidney and urinary tract infections age
67 Endoscopic procedures on female reproductive system $ 960 3970 3.8<br />
68 Neonate, admission weight 1250-1499g, without significant OR<br />
procedure $16,075 234 3.8<br />
69 Major procedures <strong>for</strong> malignant breast conditions $ 4,559 824 3.8<br />
70 Gastroenteritis age 64 $ 4,319 761 3.3<br />
84 Peripheral vascular disorder (with non-major complications) or<br />
(age >74 without complications) $ 1,919 1700 3.3<br />
85 Coronary bypass without invasive cardiac investigative procedure with<br />
major complications $18,714 174 3.3<br />
86 Renal failure with complications $ 4,079 793 3.2<br />
87 Appendectomy with complicated principal diagnosis $ 3,599 898 3.2<br />
88 Cardiac valve procedure with pump without invasive card investigative<br />
procedure with major complications $24,712 129 3.2<br />
89 Minor head injury $ 720 4374 3.1<br />
90 Other respiratory system diagnoses age >64 with complications $ 3,119 1006 3.1<br />
91 Cardiothoracic or vascular procedures <strong>for</strong> neonates $54,702 57 3.1<br />
92 Vascular procedures except major reconstruction without pump without<br />
complications $ 2,879 1082 3.1<br />
93 Vascular procedures except major reconstruction without pump with<br />
complications $ 6,958 446 3.1<br />
94 Stomach, oesophageal and duodenal procedures with non-major<br />
complications $10,557 291 3.1<br />
95 Cystic fibrosis $ 6,958 439 3.1<br />
96 Neonate, admission weight 1000-1249g, without significant<br />
OR procedure $16,075 184 3.0<br />
97 Shoulder, elbow or <strong>for</strong>earm procedures except major joint age
Top 100 Indicative prices paid by the HFA <strong>for</strong> inpatient hospital<br />
procedures ranked by discharge number<br />
Rank<br />
Diagnostic Related Group (DRG) Description<br />
National<br />
Price<br />
1999/00<br />
per patient<br />
Number <strong>of</strong><br />
Discharges<br />
Total<br />
Expenditure<br />
$million<br />
1 Abdominal pain or mesenteric adenitis without complications $ 720 7379 5.3<br />
2 Chronic obstructive airways disease $ 1,919 7368 14.1<br />
3 Bronchitis and asthma age 2499g, without significant OR procedure,<br />
without problem $ 720 6771 4.9<br />
5 Other skin, subcutaneous tissue and breast procedures $ 960 6255 6.0<br />
6 Heart failure and shock $ 2,639 6059 16.0<br />
7 Chest pain $ 960 5953 5.7<br />
8 Tonsillectomy and/or adenoidectomy $ 960 5938 5.7<br />
9 Dental extractions and restorations $ 960 5267 5.1<br />
10 Cellulitis age
38 Lower extremity and humerus procedures except hip, foot, femur<br />
age
77 Abortion without D and C $ 720 1620 1.2<br />
78 Respiratory neoplasms with complications $ 3,359 1617 5.4<br />
79 Signs and symptoms <strong>of</strong> musculoskeletal system and connective tissue<br />
age
Relationships With Communities<br />
Maintaining positive, sustainable and mutually beneficial relationships with health providers, health<br />
pr<strong>of</strong>essionals, the many organisations representing them, in fact, the tens <strong>of</strong> thousands <strong>of</strong> people working in<br />
health and community services sector 1 , requires ongoing commitment and communication on the part <strong>of</strong><br />
Personal <strong>Health</strong> staff.<br />
Transparent decision-making and using clear sets <strong>of</strong> principles to determine what services are funded is the<br />
approach the Personal <strong>Health</strong> has adopted.<br />
But initiating continuing dialogue and consulting with the communities <strong>of</strong> pr<strong>of</strong>essionals is a vital key to<br />
achieving the desired health gains <strong>for</strong> New Zealanders. Five HFA community relations managers work in<br />
the various localities to facilitate community dialogue and consultation.<br />
However, Personal <strong>Health</strong> managers play a major role in sector communication and collaboration.<br />
Expert advisors and technical committees add knowledge and depth to Personal <strong>Health</strong>’s base <strong>of</strong> expertise<br />
while also keeping communication channels open.<br />
Personal <strong>Health</strong> Senior<br />
Management Team<br />
David Moore<br />
General Manager<br />
David has a Master <strong>of</strong><br />
Commerce and a Diploma <strong>of</strong><br />
<strong>Health</strong> Economics, and has<br />
had a wide range <strong>of</strong><br />
experience in both public<br />
and private sector<br />
organisations, including the<br />
Department <strong>of</strong> <strong>Health</strong> and<br />
Treasury. He was the General Manager <strong>of</strong><br />
PHARMAC from 1993 to 1998, when he left to<br />
become the General Manager <strong>of</strong> Personal <strong>Health</strong><br />
group. He was also regional director <strong>of</strong> the<br />
Transitional <strong>Health</strong> Authority during the<br />
amalgamation <strong>of</strong> the RHAs into the HFA.<br />
David was acting joint chief executive <strong>of</strong>ficer <strong>of</strong><br />
the HFA with Kath Fox from Phil Pryke’s<br />
resignation until the appointment <strong>of</strong> Sally<br />
Wilkinson as interim chief executive <strong>of</strong>ficer.<br />
Mara Andrews<br />
Service Strategy Manager<br />
Mara has a Business Studies<br />
qualification endorsed in<br />
health management from<br />
Massey University, and has<br />
nearly completed an MBA<br />
from Henley Management<br />
College in the UK. She recently<br />
returned from a three month study visit to the USA<br />
and Canada on a World <strong>Health</strong> Organisation<br />
Fellowship, where she looked at health services <strong>for</strong><br />
indigenous people.<br />
Mara is <strong>of</strong> Ngati Kahungunu, Whakatohea, and<br />
Ngati Raukawa descent, and came to Personal<br />
<strong>Health</strong> from the HFA’s Maori <strong>Health</strong> group, where<br />
she had worked as a manager <strong>for</strong> more than five<br />
years. In that time, she was also project manager<br />
<strong>for</strong> the Napier-Hastings needs assessment.<br />
John Baird<br />
Senior Project Manager<br />
John has a background <strong>of</strong> 15<br />
years in the health sector.<br />
His initial interests were in<br />
medical research, completing<br />
a BMedSci be<strong>for</strong>e working <strong>for</strong><br />
a pharmaceutical company.<br />
He also has an MBA with<br />
an interest in service<br />
management and health sector in<strong>for</strong>mation.<br />
In 1995, John joined Coopers and Lybrand<br />
as a health sector consultant. Notable projects<br />
included hospital business planning and site<br />
configuration, a variety <strong>of</strong> hospital and primary<br />
care service development initiatives, and<br />
purchasing development work <strong>for</strong> regional<br />
health authorities.<br />
John joined the THA in 1997 to work in the primary<br />
care area, be<strong>for</strong>e being appointed to his current role<br />
in August 1998.<br />
44
Win Bennett<br />
Service Strategy Manager<br />
Win has a background <strong>of</strong><br />
twenty years in general<br />
practice. He has an MBChB<br />
and a BMedSci from Otago<br />
University. Win became<br />
interested in health policy<br />
and has almost completed an<br />
MPP from Victoria University.<br />
He was medical director <strong>of</strong> PHARMAC <strong>for</strong> five<br />
years, and briefly general manager, be<strong>for</strong>e<br />
transferring to the HFA.<br />
Win is at present focusing on primary care and<br />
service development. He has a particular interest<br />
in evidence-based purchasing, disease state<br />
management and getting the sector to work<br />
together <strong>for</strong> the benefit <strong>of</strong> patients.<br />
Chris Chadwick<br />
Planning Manager<br />
Chris has an MSc (1 st Class<br />
Hons) in mathematics from<br />
Auckland University, as well<br />
as a Diploma in <strong>Health</strong><br />
Administration from Massey<br />
University. He has <strong>for</strong>mal<br />
training in work study and<br />
method study in the health<br />
sector, and spent four years in service management<br />
in London Teaching Hospitals.<br />
His career in health management in New Zealand<br />
has included positions with the Auckland Hospital<br />
Board, Auckland Area <strong>Health</strong> Board, and North<br />
<strong>Health</strong> (the regional health authority <strong>for</strong> the<br />
northern region). He has considerable experience<br />
developing and monitoring Funding Agreements,<br />
and is currently responsible <strong>for</strong> planning and<br />
business processes within Personal <strong>Health</strong>.<br />
Peter Daws<br />
Senior Locality Manager, Christchurch<br />
Peter has an MBA, and<br />
various other qualifications in<br />
management and health<br />
services management. He has<br />
worked in health management<br />
<strong>for</strong> about 15 years, mostly in<br />
the National <strong>Health</strong> Service in<br />
Britain.<br />
His previous experience has included senior<br />
hospital administration positions at two London<br />
hospitals. At the start <strong>of</strong> the purchaser/provider<br />
re<strong>for</strong>ms in 1991, he moved to the Harrogate <strong>Health</strong><br />
Centre in north Yorkshire, where he worked until<br />
1998. In 1998, he moved to New Zealand and<br />
joined the HFA.<br />
Martin Hef<strong>for</strong>d<br />
Senior Locality Manager, Wellington<br />
Martin has a BA and<br />
Postgraduate Diploma in<br />
psychology and an MA<br />
(Applied) in social work.<br />
He worked as an advisory<br />
<strong>of</strong>ficer at the Department <strong>of</strong><br />
Social Welfare from 1986<br />
until 1991, when he became<br />
coordinator <strong>of</strong> the Wellington branch <strong>of</strong> the<br />
Schizophrenia Fellowship. In this position, he<br />
managed a community activity centre, and respite<br />
care, education and support services <strong>for</strong> people with<br />
serious mental illness and their families.<br />
He joined the newly established Central RHA in<br />
1993 as a disability support services analyst,<br />
and managed the deinstitutionalisation <strong>of</strong> Porirua<br />
Hospital. In 1995, Martin was appointed to manage<br />
the new Mental <strong>Health</strong> group when the RHA<br />
restructured, and became the Personal <strong>Health</strong><br />
senior locality manager in 1998.<br />
Julian Inch<br />
Service Strategy Manager<br />
Julian has qualifications<br />
in economics, systems<br />
modelling and management<br />
to postgraduate level. He has<br />
worked in the <strong>Ministry</strong> <strong>of</strong><br />
<strong>Health</strong> as a senior economist<br />
and manager in the health<br />
policy and funding area,<br />
as well as both Wellington Hospital and<br />
Canterbury <strong>Health</strong>.<br />
He joined the HFA in 1998, and has a strong interest<br />
in improving its purchasing functions. He and his<br />
team have focused on putting national purchase<br />
frameworks and developing prioritisation,<br />
contracting and monitoring tools and processes.<br />
Julian has built close relationships with key sector<br />
groups and stakeholders, and the service strategy<br />
team has a good reputation in the sector.<br />
HFA Improving Our <strong>Health</strong> 45
Sue Keppel<br />
Senior Locality Manager, Auckland<br />
Sue has an LLB (Hons) and<br />
an MJur (Distinction) and<br />
is a registered general<br />
and obstetric nurse.<br />
She has had considerable<br />
experience in the health<br />
sector, both funding health<br />
services and working <strong>for</strong> a<br />
variety <strong>of</strong> providers.<br />
In her current position as senior locality manager,<br />
Sue is responsible <strong>for</strong> Personal <strong>Health</strong> contracts in<br />
the Auckland and Northland areas.<br />
David Pearson<br />
Finance Manager<br />
David has an MBA and a<br />
BCom in accounting, and is<br />
a member <strong>of</strong> the Institute <strong>of</strong><br />
Chartered Accountants <strong>of</strong><br />
New Zealand. Prior to<br />
joining the HFA in 1998,<br />
he was the Director <strong>of</strong><br />
Finance <strong>for</strong> the New Zealand<br />
Customs Service, where he was responsible <strong>for</strong><br />
corporate finance services.<br />
He has also been an associate partner with BDO<br />
Hogg Young Cathie, a chartered accountancy firm,<br />
a contractor in finance roles in England, and an<br />
auditor with Coopers and Lybrand.<br />
Grant Ramsay<br />
IM Manager<br />
Grant has worked in<br />
in<strong>for</strong>mation systems <strong>for</strong> the<br />
HFA and its predecessors<br />
since 1994. He has a BCom<br />
from Canterbury University<br />
and is completing a Graduate<br />
Diploma <strong>of</strong> Business<br />
in in<strong>for</strong>mation systems<br />
at Auckland University.<br />
In his in<strong>for</strong>mation systems roles, Grant has<br />
implemented contract management, client<br />
enrolment and payment processing systems, lead<br />
the integration <strong>of</strong> North <strong>Health</strong> operations into<br />
national HFA and HBL operations, and managed a<br />
development group <strong>of</strong> 40 during the transition from<br />
RHAs to the HFA. His current role focuses on key<br />
strategic in<strong>for</strong>mation management and business<br />
process developments, including those <strong>of</strong> HBL.<br />
Ross Smith<br />
Senior Locality Manager, Hamilton<br />
Ross has a BCom from<br />
Canterbury University, and<br />
has had extensive experience<br />
in senior commercial roles in<br />
the manufacturing sector.<br />
He joined Midland RHA as<br />
a contract relationship<br />
manager in 1993. In 1998,<br />
he was appointed as senior<br />
locality manager <strong>for</strong> the Personal <strong>Health</strong> group.<br />
Since 1993, he has been involved in major provider<br />
contract negotiations, <strong>of</strong>ten involving significant<br />
change management and community consultation.<br />
He has extensive networks with the local<br />
communities and providers served by the Hamilton<br />
<strong>of</strong>fice, and wide experience in developing local<br />
solutions to improve health service delivery.<br />
Other senior managers<br />
Gillian Bohm<br />
Quality Auditor<br />
Gillian is responsible <strong>for</strong><br />
audit and quality<br />
improvement programmes in<br />
hospitals and health services.<br />
She has welcomed the<br />
opportunity to articulate<br />
quality imperatives <strong>for</strong> public<br />
hospitals and to initiate<br />
projects that address national deficits in the<br />
provision <strong>of</strong> safe care.<br />
She was involved in a project to review systems <strong>for</strong><br />
checking the credentials <strong>of</strong> medical practitioners<br />
that is accepted by the sector and will be used in<br />
the development <strong>of</strong> a national framework and<br />
process to be extended to other pr<strong>of</strong>essional groups.<br />
Gillian was also involved in auditing HHS systems<br />
<strong>for</strong> reporting incidents. This audit provided the<br />
in<strong>for</strong>mation <strong>for</strong> a guideline <strong>for</strong> reportable events<br />
in HHSs.<br />
46
Barbara Browne<br />
Maternity Advisor<br />
Barbara is a registered nurse<br />
and has a BA and an LLB<br />
(Hon). She is responsible <strong>for</strong><br />
leading the maternity<br />
services review, developing<br />
the HFA’s future maternity<br />
strategy, and maintaining<br />
present maternity contracts.<br />
She works with consumer, provider, and<br />
pr<strong>of</strong>essional groups to deliver high quality and<br />
coordinated services. Her role is split between the<br />
service strategy team and the Auckland and<br />
Hamilton locality teams.<br />
She has previously worked as a nurse and<br />
operational manager in hospitals, an educator <strong>for</strong><br />
a postgraduate nursing and midwifery course,<br />
a health sector union organiser, and a locality<br />
manager <strong>for</strong> the Midland RHA.<br />
Gabrielle Collison<br />
Clinical Advisor<br />
Gabrielle has an MBChB,<br />
DPH, and DIH, and is a<br />
Fellow <strong>of</strong> the Australasian<br />
Faculty <strong>of</strong> Public <strong>Health</strong><br />
Medicine. She is the<br />
northern regional director <strong>of</strong><br />
training <strong>for</strong> the AFPHM, and<br />
has a long history <strong>of</strong> working<br />
in public health medicine in New Zealand.<br />
In her current role, she is the leader <strong>of</strong> the child<br />
health project and chair <strong>of</strong> the paediatric specialty<br />
services review group. She has been involved in<br />
the development <strong>of</strong> the child health business plan<br />
to implement the child health strategy, grouping<br />
all HFA child health workstreams to improve<br />
linkages, and addressing service delivery,<br />
configuration and work<strong>for</strong>ce issues such as in<br />
paediatric oncology services.<br />
Sandy Dawson<br />
Chief Clinical Advisor<br />
Sandy is a doctor with postgraduate qualifications<br />
in occupational medicine and aviation medicine,<br />
and is a Fellow <strong>of</strong> the Australasian Faculty <strong>of</strong> Public<br />
<strong>Health</strong> Medicine. He has worked <strong>for</strong> the RNZAF<br />
and Air New Zealand,<br />
looking at how people<br />
per<strong>for</strong>m in stressful<br />
environments. He then<br />
worked at ACC as their<br />
corporate medical advisor.<br />
He is part <strong>of</strong> the team<br />
working on developing disease-state approaches,<br />
especially in diabetes, and provides clinical input<br />
<strong>for</strong> high-cost treatment and prioritisation processes.<br />
Sandy promotes having more clinician and<br />
consumer input to maximise the focus on getting<br />
the best value from the funding available.<br />
Martin de Boer<br />
Team Leader, Service In<strong>for</strong>mation<br />
Martin has a BSc in<br />
operations research and a<br />
Diploma <strong>of</strong> Public <strong>Health</strong>.<br />
His previous work experience<br />
has included independent<br />
contracting work <strong>for</strong> the<br />
HFA, consultant at KPMG,<br />
and statistician <strong>for</strong> the<br />
Analysis and Monitoring Unit <strong>of</strong> the Public <strong>Health</strong><br />
Commission.<br />
In his current role, Martin’s key responsibilities<br />
include monitoring and leading the service<br />
in<strong>for</strong>mation team. His most recent projects have<br />
been on HHS purchasing and the national<br />
minimum dataset.<br />
Laura Lambie<br />
Clinical Advisor<br />
Laura is a registered nurse<br />
and midwife, with additional<br />
qualifications in education<br />
and public health. Be<strong>for</strong>e she<br />
joined the HFA, she has<br />
worked on major reviews at<br />
Capital Coast <strong>Health</strong>,<br />
maternity research through<br />
Otago University, education <strong>of</strong> health pr<strong>of</strong>essionals,<br />
and work in management and as a health<br />
pr<strong>of</strong>essional.<br />
In her current role, Laura is responsible <strong>for</strong><br />
developing a national strategy <strong>for</strong> funding palliative<br />
care. The palliative care project will eventually<br />
HFA Improving Our <strong>Health</strong> 47
esult in nationally consistent palliative care<br />
services being available <strong>for</strong> all New Zealanders.<br />
She is also responsible <strong>for</strong> developing a strategy<br />
<strong>for</strong> purchasing cardiac services within a disease<br />
management approach.<br />
Julie Martin<br />
Project Manager<br />
Julie is a registered general<br />
and obstetric nurse, and has<br />
a Diploma in Business<br />
Studies and an Advanced<br />
Diploma in Nursing. She is<br />
currently completing a<br />
Masters <strong>of</strong> <strong>Health</strong><br />
Management through Massey<br />
University. Her key area <strong>of</strong> interest is in improving<br />
health sector management, especially in primary<br />
and community care.<br />
Prior to joining the HFA, Julie worked <strong>for</strong> the<br />
Auckland Methodist Mission Aged Care Services,<br />
where she established their in-service training<br />
department and implemented organisation-wide<br />
quality management programmes. She is currently<br />
responsible <strong>for</strong> the Hepatitis B, integrated care, rural<br />
health and diabetes projects.<br />
Tracy Mellor<br />
Team Leader, Quality and Audit<br />
Tracy has a BA in<br />
developmental psychology,<br />
and is a Fellow <strong>of</strong> the<br />
Chartered Institute <strong>of</strong><br />
Housing. Be<strong>for</strong>e joining the<br />
Central RHA, she had<br />
extensive experience in<br />
public sector housing<br />
management in England, and developed particular<br />
expertise in the development and monitoring <strong>of</strong><br />
contracts.<br />
In her first position at the RHA, Tracy was<br />
responsible <strong>for</strong> child and adolescent health services.<br />
Following the amalgamation <strong>of</strong> the RHAs into the<br />
HFA, Tracy was appointed team leader <strong>of</strong> the quality<br />
and audit team. She has been responsible <strong>for</strong> the<br />
management and co-ordination <strong>of</strong> the HFA’s<br />
investigation into the allegations <strong>of</strong> cervical smear<br />
misreading in Gisborne.<br />
Valerie Meyer<br />
Project Manager<br />
Valerie is a registered<br />
comprehensive nurse, and<br />
has extensive experience in<br />
both clinical and<br />
management roles within the<br />
health sector in New Zealand<br />
and overseas. Her most<br />
recent position be<strong>for</strong>e joining<br />
the HFA was with ACC, where she developed a<br />
sound base <strong>of</strong> experience in case management,<br />
project management, change management, and<br />
other areas.<br />
Valerie is the team leader <strong>of</strong> the waiting times<br />
project, and as such has been involved in the<br />
development and implementation <strong>of</strong> booking<br />
systems <strong>for</strong> elective procedures.<br />
Marama Parore-Katene<br />
Clinical Advisor<br />
Marama is a registered nurse,<br />
with experience working<br />
with Te Kohanga Reo, Maori<br />
Women’s Welfare League, the<br />
Public <strong>Health</strong> Commission<br />
and Plunket. At the Public<br />
<strong>Health</strong> Commission, she was<br />
the national immunisation<br />
and glue ear educator, with responsibility <strong>for</strong><br />
developing health education resources. She was<br />
the Maori area manager and national Maori clinical<br />
educator <strong>for</strong> Plunket, and developed Plunket’s<br />
Kaiawhina course and standards <strong>of</strong> practice.<br />
Marama joined the Central RHA as a programme<br />
and relationship manager, responsible <strong>for</strong> IPA and<br />
Maori provider contract management. She then<br />
moved to the Maori <strong>Health</strong> group, be<strong>for</strong>e joining<br />
the Personal <strong>Health</strong> service strategy team. She is<br />
<strong>of</strong> Ngati Whatua, Ngati Kahu, and Ngati Wai<br />
descent.<br />
Sue Peacock<br />
Project Manager<br />
Sue has a Masters in Clinical Pharmacy with Credit<br />
from Otago University. She is a Fellow <strong>of</strong> the<br />
Society <strong>of</strong> Hospital Pharmacists <strong>of</strong> Australia, and a<br />
48
member <strong>of</strong> the<br />
Pharmaceutical Society <strong>of</strong><br />
New Zealand. She has been<br />
chief executive <strong>of</strong> the<br />
Pharmacy Guild <strong>of</strong><br />
New Zealand.<br />
Be<strong>for</strong>e joining the HFA, Sue<br />
worked as an independent contractor, working on<br />
a variety <strong>of</strong> primary care projects <strong>for</strong> the<br />
Transitional <strong>Health</strong> Authority and RHAs.<br />
She is currently team leader <strong>of</strong> the primary care<br />
project, and has successfully managed the<br />
development and implementation <strong>of</strong> new primary<br />
care contracts under a national framework.<br />
Philip Pigou<br />
Project Manager<br />
Philip has an LLB from<br />
Canterbury University and a<br />
Diploma <strong>of</strong> Business Studies<br />
from Massey University.<br />
He is also a qualified tenancy<br />
mediator, and was admitted<br />
to the High Court as a<br />
barrister and solicitor in<br />
1983. He has worked <strong>for</strong> a variety <strong>of</strong> government<br />
departments, including the Department <strong>for</strong> Courts<br />
and Housing New Zealand.<br />
Philip manages the laboratory services project,<br />
developing purchasing strategies <strong>for</strong> community<br />
laboratory services. He also managed the project<br />
to transfer post-mortem funding and purchasing<br />
to the Department <strong>for</strong> Courts. He has been involved<br />
in negotiating the national primary care contract<br />
and the <strong>Health</strong>line contract.<br />
Ruth Rhodes<br />
Clinical Advisor<br />
Ruth is a registered nurse,<br />
with postgraduate diplomas<br />
in public health, nursing, and<br />
social work. She has<br />
previously worked in health<br />
promotion and public health<br />
nursing at <strong>Health</strong> Waikato.<br />
In Ruth’s current position,<br />
she is responsible <strong>for</strong> the national Tamariki Ora/<br />
Well Child project and implementation <strong>of</strong> new<br />
funding <strong>for</strong> child health services. She is involved<br />
in relationship management and contract<br />
negotiation with numerous health providers,<br />
including Plunket, and also oversees dental and<br />
rural health services <strong>for</strong> the Hamilton locality team.<br />
David Sinclair<br />
Clinical Advisor<br />
David is a doctor, with<br />
specialist qualifications in<br />
public health. He recently<br />
joined Personal <strong>Health</strong><br />
from the HFA’s Public<br />
<strong>Health</strong> group, where he<br />
was a portfolio manager,<br />
with responsibility <strong>for</strong><br />
immunisation. Prior to that, he was medical <strong>of</strong>ficer<br />
<strong>of</strong> health <strong>for</strong> <strong>Health</strong> Waikato.<br />
In his current position as clinical advisor, David is<br />
responsible <strong>for</strong> developing national strategies in<br />
immunisation and sexual health services. Moves<br />
to improve immunisation have been gaining<br />
momentum through the HFA’s child health business<br />
plan, and David will help to carry this through into<br />
developing programmes and services. He also<br />
provides clinical advice on a number <strong>of</strong> other areas.<br />
Ruth Stannard<br />
Team Leader, Advanced Contracting<br />
Ruth has a BBS in economics,<br />
and has had five years’<br />
experience in the health<br />
sector. Be<strong>for</strong>e joining<br />
the HFA, she worked at<br />
the <strong>Ministry</strong> <strong>of</strong> <strong>Health</strong><br />
as an economic advisor,<br />
responsible <strong>for</strong> providing<br />
advice to the Government on sector structures,<br />
risk management, and budget initiatives.<br />
Her current role focuses on pharmacy and oral<br />
health services. She led the team that developed<br />
the HFA’s purchase plan and consultation document<br />
<strong>for</strong> child and adolescent oral health services, and<br />
is currently consulting with the pharmacy sector<br />
on access to new contracts.<br />
1 Some 109,320 people are employed in the health and community<br />
services industry sector, Statistics Department, 1998.<br />
HFA Improving Our <strong>Health</strong> 49
Personal <strong>Health</strong> - External Advisory<br />
Groups and Committees<br />
Personal <strong>Health</strong> seeks advice and guidance from a<br />
wide range <strong>of</strong> stakeholder groups and the<br />
community. The following is a list <strong>of</strong> people<br />
providing advice to Personal <strong>Health</strong> or taking part<br />
in joint working parties with Personal health.<br />
HFA participants on joint working parties are not<br />
included.<br />
Travel and Accommodation Assistance Policy<br />
HHS Advisory Group<br />
Ian Anderson, Streamliners / Canterbury<br />
Tracey Adamson, <strong>Health</strong>Care Hawkes Bay<br />
Paul Greertson, Good <strong>Health</strong> Wanganui<br />
Maree Neville, Capital Coast <strong>Health</strong><br />
Kerry Farmer, Pacific <strong>Health</strong><br />
John Phibbs, Auckland <strong>Health</strong>care<br />
John Mitchell, <strong>Health</strong> Link South<br />
Harry Barber, Tairawhiti <strong>Health</strong>care<br />
Fiona Robertson, Canterbury <strong>Health</strong><br />
Wider Sector Advisory Group<br />
Helen Sullivan, National Cancer Society<br />
Margaret Hood, National Heart Foundation<br />
Jacqui Te Kani, Maori Women’s Welfare League<br />
Ruth Nepia / Rahira Walsh, Maori <strong>Health</strong><br />
Commission<br />
Heather Simspon, Schizophrenia Fellowship NZ Inc<br />
Margaret Hamilton, Mental <strong>Health</strong> Consumer<br />
Consultant<br />
Elizabeth Cooper, Assembly <strong>of</strong> People with<br />
Disabilities<br />
Richard Buchanan, NZCCS<br />
Taima Campbell, Clinical Manager - Te Waka Hauora<br />
Sandra Murphy, Starship Children’s Hospital<br />
Keith Grimwood, Wellington School <strong>of</strong> Medicine -<br />
Paediatric Review Group<br />
Emergency Services - MoH and HHSs<br />
Ian Civil, Auckland <strong>Health</strong>care Trauma Surgeon<br />
Ge<strong>of</strong>f Hughes, Capital Coast <strong>Health</strong> Emergency<br />
Medicine Specialist<br />
Jim Ross, Ox<strong>for</strong>d GP<br />
Sarah Little, Starship ED nurse<br />
John Ayling, CEO Ambulance Board<br />
Anne-Marie van der Linden, ACC<br />
Deborah Woodley, MoH<br />
Diabetes<br />
Paul Curry, Chair Wellington Diabetes team<br />
Dr Jo Baxter, Maori Doctors Ti Ora<br />
Valerie Brown, Maori Provider<br />
Dr Jan Bryant, Maori GP<br />
Dr Kirsten Coppell, Public <strong>Health</strong> specialist<br />
Dr Rick Cutfield, Diabetes specialist<br />
Norma Haley, Diabetes Youth<br />
Margaret Jamieson, Diabetes New Zealand<br />
Dr Tim Kenealy, GP<br />
Dr Helen Lunt, Diabetes specialist<br />
June Swindells, Maori provider<br />
Maxine Tangihaere, Maori Provider<br />
Dr Colin Tukuitonga, PI public health<br />
Suzy Whitcombe, Diabetes nurse educator<br />
Donna Richards, Te Roopu Mate Huka<br />
Dr Ashley Bloomfield, MoH<br />
Tamariki Ora/Well Child and Immunisation<br />
Technical Advisory Group<br />
Angela Baldwin, Plunket Society, Wellington<br />
Anna Bailey, <strong>Health</strong> Star Pacific<br />
Brett Austin, Plunket Society, Auckland<br />
Carol Stott, Child <strong>Health</strong> & Family Services<br />
Auckland <strong>Health</strong>care<br />
Dr Tueila Percival, C/- Middlemore Hospital<br />
Matapihi Kingi, Tipu Ora Rotorua<br />
Matea Gillies, Ngai Tahu<br />
Q. Mahanga, Hauora Whanui<br />
Marion Guy, NZNO Practice Nurse<br />
Nick Baker, Paediatric Society<br />
Pat Tuohy, <strong>Ministry</strong> <strong>of</strong> <strong>Health</strong><br />
50
Dr Tim McKenzie, GP Wellington, NZMA<br />
Reg Ratahi, Waipairera Trust<br />
Morehu MacDonald<br />
Palliative Care - HHSs, NHSC, Hospice providers<br />
and community interest groups<br />
Dr Rod McLeaod, Mary Potter Hospice<br />
Ms Jan Nichols, St Josephs Hospice<br />
Ms Robin Steed, <strong>Health</strong> Waikato<br />
Ms Janice Wenn, Whaiora Whanui<br />
Dr Mark Jeffery, Canterbury <strong>Health</strong><br />
Ms Maggie Barry<br />
Dr Brian King, GP<br />
Mr Mervyn Monk, Hospice NZ<br />
Roadside To Bedside Emergencies Focus Group<br />
Maggie Banks, NZCOM<br />
Ann Yates, NZCOM<br />
Heather Muriwai, NZCOM<br />
Tim Malloy<br />
Barbara Beck<strong>for</strong>d<br />
Rob Sinclair, The Order <strong>of</strong> St John<br />
Miriama Kupe, Nga Maia<br />
Corrina Vaughan, Nga Maia<br />
Al Haslam, NZMA<br />
Phil Weston, NZMA<br />
Ultrasound Utilisation Review Committee<br />
Carey Virtue, NZCOM<br />
Sandy Grey, NZCOM<br />
Teenah Handiside, Federation <strong>of</strong> Women’s <strong>Health</strong><br />
Councils<br />
Graham Parry, NZMA<br />
Robert Sim, RANZ College <strong>of</strong> Radiologists<br />
Dr Nigel Anderson, RANZ College <strong>of</strong> Radiologists<br />
Miriama Kupe, Nga Maia<br />
Joanne Rama, Nga Maia<br />
Dominic Stayne (analyst <strong>for</strong> committee)<br />
Paediatric Specialty Services Review Project<br />
Group<br />
Dr Nick Baker, Paed Society<br />
Pr<strong>of</strong> Barry Taylor, Paed Society<br />
Dr Scott McFarlane, Paed Society<br />
Pr<strong>of</strong> Keith, Grimwoodd Paed Society<br />
Dr Adrian, Trenholme Paed Society<br />
Dr Pat Touhy, MoH<br />
Nicky Shave, Nurses Advisory Group<br />
Technical Working Groups within<br />
<strong>Health</strong> and Hospital Services<br />
The HFA has <strong>for</strong>med a large number <strong>of</strong> Technical<br />
Working groups with HHS. These comprise HFA<br />
and HHS staff as follows:<br />
Pricing Group (Price Path)<br />
Determines aggregate start point <strong>of</strong> HHS revenue<br />
(based on 1999/2000 actual) and the price path<br />
<strong>for</strong>ward to aggregate 2000/2001 revenue. Price path<br />
is the net <strong>of</strong> an inflation adjuster and an allowance<br />
<strong>for</strong> efficiency gains in the sector.<br />
Nigel Dewar, Lakeland <strong>Health</strong><br />
Stuart Powell, HFA<br />
Andrew Gaudin, CHA<br />
Chris Hoar, Canterbury <strong>Health</strong><br />
Sally Rennie, HFA<br />
Weiguo Ding, HFA<br />
Justine Tringham, Auckland <strong>Health</strong>care<br />
Chris Dyhrberg, Capital Coast <strong>Health</strong><br />
David Green, HFA<br />
John Bates, HFA<br />
Nigel Cunningham, Coast <strong>Health</strong> Care<br />
Peter McIntosh, Coast <strong>Health</strong> Care<br />
David Chrisp, HFA<br />
Base Volumes<br />
Provides a variety <strong>of</strong> volume data sets (eg contract,<br />
actual, national intervention rates) to in<strong>for</strong>m the<br />
discussions between localities and HHSs to arrive<br />
at 2000/2001 contract volumes.<br />
Julie Wilson, <strong>Health</strong> Waikato<br />
Martin de Boer, HFA<br />
Dr Gary Jackson, South Auckland <strong>Health</strong><br />
Ge<strong>of</strong>frey Forbes, HFA<br />
Owen Wallace, Pacific <strong>Health</strong><br />
Jan Parker, HFA<br />
Mark Spittal, Canterbury <strong>Health</strong><br />
HFA Improving Our <strong>Health</strong> 51
Shane Davidson, Canterbury <strong>Health</strong><br />
Ron Craft, HFA<br />
Nigel Kee, HFA<br />
Paul Howard, HFA<br />
Ian Westbrooke, HFA<br />
Joy Christison, HFA<br />
Mark Batt, HFA<br />
Elizabeth Butturini, Hutt Valley <strong>Health</strong><br />
Zoran Bolevich, Good <strong>Health</strong> Wanganui<br />
Tim Wood, HFA<br />
Janice Donaldson, HFA<br />
Jesse Kokaua, HFA<br />
Cliff la Grange, Waitemata <strong>Health</strong><br />
Dr Phil Hider, Department <strong>of</strong> Public <strong>Health</strong> and<br />
General Practice, Christchurch School <strong>of</strong> Medicine<br />
Capital Cost<br />
Proposes a way <strong>of</strong> incorporating depreciation,<br />
interest and capital cost into prices.<br />
Andrew Gaudin, CHA<br />
Stuart Powell, HFA<br />
Graeme Edmond, Auckland <strong>Health</strong>care Services<br />
Ian Ward, Auckland <strong>Health</strong>care Services<br />
Warren Young, Hutt Valley <strong>Health</strong><br />
Jonathon Jourdain, HFA<br />
Steve Anderson, CCMAU<br />
Chris Fleming, <strong>Health</strong>care Hawkes Bay<br />
Ian Ward, Auckland <strong>Health</strong>care<br />
Murray Gerogel, Midcentral <strong>Health</strong><br />
Peter Beirne, Midcentral <strong>Health</strong><br />
Chai Chuah, Canterbury <strong>Health</strong><br />
Rochelle Leahy, Hutt Valley <strong>Health</strong><br />
Andrew Powell, Capital Coast <strong>Health</strong><br />
Terry kendall, <strong>Health</strong> Waikato<br />
Nigel Dewar, Lakeland <strong>Health</strong><br />
Pranay Lodhiya, Good <strong>Health</strong> Wanganui<br />
Perry Kendall, <strong>Health</strong> Waikato<br />
Benchmarking (an HHS project)<br />
Identify sector benchmarking objectives and<br />
develop a proposal to meet them.<br />
Brenda Bromell, <strong>Health</strong> Waikato<br />
Gary Koppes, Coast <strong>Health</strong> Care<br />
Fay Logan, <strong>Health</strong>link South<br />
Zoran Bolevich, Good <strong>Health</strong> Wanganui<br />
Rosemary Jarmey , Capital Coast <strong>Health</strong><br />
Darma Black, Capital Coast <strong>Health</strong><br />
Leigh Monks, Good <strong>Health</strong> Wanganui<br />
Megan Boivin, <strong>Health</strong>care Otago<br />
Teresa Chalecki, Coast <strong>Health</strong> Care<br />
Sharon Pearce, South Auckland <strong>Health</strong><br />
Elizabeth Butturini, Hutt Valley <strong>Health</strong><br />
Andrew Powell, Capital Coast <strong>Health</strong><br />
Helen Wood, HFA<br />
Brent Wiseman, <strong>Health</strong> Waikato<br />
Jim Knight, South Auckland <strong>Health</strong>care<br />
Michael Rains, HFA<br />
Tony Hickmott, Auckland <strong>Health</strong>care<br />
Bottom up costing (an HHS project)<br />
Seeks to compare relative per<strong>for</strong>mance <strong>of</strong> HHSs<br />
based on costing in<strong>for</strong>mation derived from HHSs<br />
using the common costing standards.<br />
Leigh Monks, Good <strong>Health</strong> Wanganui<br />
Roy Chan, HFA<br />
Roger Lamond, <strong>Health</strong>link South<br />
Paul Taumanu, <strong>Health</strong> Waikato<br />
Ron Craft, HFA<br />
Pranay Lodhiya, Good <strong>Health</strong> Wanganui<br />
Nigel Cunnigham, Coast <strong>Health</strong> Care<br />
Sally Rennie, HFA<br />
Elizabeth Butturini, Hutt Valley <strong>Health</strong><br />
Rosemary Jarmey , Capital Coast <strong>Health</strong><br />
Julie Wilson, <strong>Health</strong> Waikato<br />
Glen Munro, HFA<br />
Maureen Chrystal, Auckland <strong>Health</strong>care<br />
Common costing standards (an HHS project)<br />
Seeks to provide HHS product cost data that can<br />
be used to in<strong>for</strong>m pricing and benchmark<br />
per<strong>for</strong>mance.<br />
Leo Hulme, <strong>Health</strong>link South<br />
Roger Lamond, <strong>Health</strong>link South<br />
Roy Chan, HFA<br />
52
Sally Rennie, HFA<br />
Glen Munro, HFA<br />
Jim Knight, South Auckland<br />
Maureen Chrystal, Auckland <strong>Health</strong>care<br />
Paul Conder, Pacific <strong>Health</strong><br />
Harry Barber, Tarawhiti <strong>Health</strong>care<br />
Chris Fleming, <strong>Health</strong>care Hawkes Bay<br />
Leigh Monks, Good <strong>Health</strong> Wanganui<br />
Elizabeth Butturini, Hutt Valley <strong>Health</strong><br />
Janice Bromell, Nelson-Marlborough <strong>Health</strong><br />
Ray Anton, <strong>Health</strong>care Otago<br />
Rod Brown, Southern <strong>Health</strong><br />
Andrew Boyd, Deloitte<br />
Andrew Gaudin, CCMAU<br />
Cost weights<br />
Aims to improve cost weights (inpatient and<br />
outpatient) used in HHS prices<br />
Michael Rains, HFA<br />
Rochelle Leahy, Hutt Valley <strong>Health</strong><br />
Leo Hulme, <strong>Health</strong>link South<br />
Alistair Ayto, South Auckland <strong>Health</strong><br />
Roy Chan, HFA<br />
Sally Rennie, HFA<br />
Weiguo Ding, HFA<br />
Estelle Muller, HFA<br />
David Green, HFA<br />
Brenda Bromell, <strong>Health</strong> Waikato<br />
John Bates, HFA<br />
Kevin Sharkey, Capital Coast <strong>Health</strong><br />
Martin de Boer, HFA<br />
Joy Christison, HFA<br />
Nigel Trainor, Nelson-Marlborough<br />
Gina Banfield, Auckland <strong>Health</strong>care<br />
Linda Fletcher, Auckland <strong>Health</strong>care<br />
Clinical Training Agency<br />
Aims to improve CTA prices in respect <strong>of</strong> the<br />
allowance <strong>for</strong> overhead costs built into prices and<br />
a price path adjustment.<br />
Tony MacDonald, <strong>Health</strong>link South<br />
Elizabeth Butturini, Hutt Valley <strong>Health</strong><br />
Data Improvement and Management<br />
Aims to identify and resolve HHS sector data issues<br />
Chris Hoar, Canterbury <strong>Health</strong><br />
Martin de Boer, HFA<br />
Ian Westbrooke, HFA<br />
Darren Wilson, <strong>Health</strong>link South<br />
Elizabeth Butturini, Hutt Valley <strong>Health</strong><br />
Maureen Chrystal, Auckland <strong>Health</strong>care<br />
Kevin Sharkey, Capital Coast <strong>Health</strong><br />
Glenys Checchi, Capital Coast <strong>Health</strong><br />
Sean Callis, HFA<br />
David Scott, HFA<br />
Warren Jackson, Good <strong>Health</strong> Wanganui<br />
Mark Batt, HFA<br />
Marjorie Anderson, South Auckland <strong>Health</strong><br />
Paul Howards, HFA<br />
Brenda Bromell, <strong>Health</strong> Waikato<br />
Jenny Murray, Taranaki <strong>Health</strong><br />
Robyn MacIntosh, HFA<br />
Jason Whakaari, HFA<br />
Janice Brommel, Nelson-Marlborough<br />
Helen Watson, HFA<br />
Gina Banfield, Auckland <strong>Health</strong>care<br />
<strong>Health</strong> and Disability Sector Standards<br />
Aims to assess the impact <strong>of</strong> the implementation<br />
<strong>of</strong> <strong>Health</strong> and Disability sector standards on HHSs<br />
and to prepare a guide to assist their effective<br />
adoption within the sector<br />
Janice Lavelle, <strong>Health</strong>link South<br />
Jane Cartwright, <strong>Health</strong>link South<br />
Raewyn Wolcke, Auckland <strong>Health</strong>care<br />
New Purchasing Approaches<br />
Aims to identify a ‘toolkit’ <strong>of</strong> new purchasing<br />
approaches<br />
Jane Parfitt, <strong>Health</strong>link South<br />
Neil Woodhams, Auckland <strong>Health</strong>care<br />
Patient Transfer<br />
Helen Wood, HFA<br />
John Phibbs, Auckland <strong>Health</strong>care<br />
HFA Improving Our <strong>Health</strong> 53
John Mitchell, <strong>Health</strong>link South<br />
Tracey Adamson, <strong>Health</strong>care Hawkes Bay<br />
Clare Connell, HFA<br />
Harry Barber, Tairawhiti <strong>Health</strong>care<br />
Lisa Lim, HFA<br />
Fiona Robertson, Canterbury <strong>Health</strong><br />
Naree Nevill, Capital Coast <strong>Health</strong><br />
Paul Greertson, Good <strong>Health</strong> Wanganui<br />
Denise Clement, Nelson-Marlborough<br />
Purchase Units and Service Specifications<br />
Develops purchase units and service specifications<br />
consistent with a set <strong>of</strong> national principles.<br />
Chris Crane, HFA<br />
Wendy Hoskin, <strong>Health</strong> Waikato<br />
Loraine Milne, HFA<br />
Roger Lamond, <strong>Health</strong>link South<br />
Elizabeth Butturini, Hutt Valley <strong>Health</strong><br />
Trish McFadden, Capital Coast <strong>Health</strong><br />
Jan Barber, HFA<br />
Kristin Wilkinson, South Auckland <strong>Health</strong><br />
Sally Rennie, HFA<br />
Marin de Boer, HFA<br />
Robbie Thomson, HFA<br />
Peter McIntosh, Coast <strong>Health</strong> Care<br />
Rosalie percival, HFA<br />
Chris Lowry, Good <strong>Health</strong> Wanganui<br />
Wendy Beverley, Capital Coast <strong>Health</strong><br />
Louise Carr, HFA<br />
Helen Watson, HFA<br />
Michael Rains, HFA<br />
Gina Banfield, Auckland <strong>Health</strong>care<br />
Rural/diseconomy<br />
Aims to identify ways <strong>of</strong> compensating HHSs <strong>for</strong><br />
costs related to the provision <strong>of</strong> services in rural<br />
areas and incurring diseconomies <strong>of</strong> scale that are<br />
not adequately reflected in the national price book.<br />
Julie Rodgers, Nelson Marlborough<br />
Helen Wood, HFA<br />
Robin Steed, <strong>Health</strong> Waikato<br />
Nigel Dewar, Lakeland <strong>Health</strong><br />
Robbie Thompson, HFA<br />
Harry Barber, Tairawhiti <strong>Health</strong>care<br />
Bev O’Cain, <strong>Health</strong>link South<br />
Nigel Kee, HFA<br />
Pranay Lodhiya, Good <strong>Health</strong> Wanganui<br />
Weiguo Ding, HFA<br />
Rod Brown, Southern <strong>Health</strong><br />
Nigel Trainor, Nelson Marlborough<br />
Michael Rains, HFA<br />
Tertiary adjuster<br />
Aims to identify ways <strong>of</strong> compensating HHSs <strong>for</strong><br />
costs related to the provision <strong>of</strong> tertiary services<br />
that are not adequately reflected in the national<br />
price book.<br />
Chris Dyhrberg, Capital Coast <strong>Health</strong><br />
Jonathon Jourdain, HFA<br />
Justine Tringham, Auckland <strong>Health</strong>care<br />
Sean Callis, HFA<br />
Julie Wilson, <strong>Health</strong> Waikato<br />
Dr Gary Jackson, South Auckland <strong>Health</strong><br />
Bob Bishop, HFA<br />
David Green, HFA<br />
Lisa Lim, HFA<br />
John Bates, HFA<br />
Kevin Sharkey, Capital Coast <strong>Health</strong><br />
Weiguo Ding, HFA<br />
Roger Lamond, <strong>Health</strong>link South<br />
Leo Hulme, <strong>Health</strong>link South<br />
Janice Lavelle, <strong>Health</strong>link South<br />
Jane Cartwright, <strong>Health</strong>link South<br />
Elizabeth Butturini, Hutt Valley <strong>Health</strong><br />
Nigel Trainor, Nelson Marlborough<br />
Michael Rains, HFA<br />
Maureen Chrystal, Auckland <strong>Health</strong>care<br />
Service Reviews<br />
A “Service” is an identifiable health or disability<br />
service, or part there<strong>of</strong>, which a health provider is<br />
funded to deliver to specified consumers. It may<br />
be a defined health service such as oral health<br />
services or defined population based health service<br />
such as child health services, or a defined service<br />
in a geographic area such as immunisation services<br />
54
in Hawkes Bay. It may only be a component <strong>of</strong><br />
one <strong>of</strong> these services, or a combination.<br />
Roy Chan, HFA<br />
Loraine Milne, HFA<br />
Margaret Ann Irwin, HFA<br />
Tim Wood, HFA<br />
Jan Barber, HFA<br />
Fiona Robertson, Canterbury <strong>Health</strong><br />
Joy Christison, HFA<br />
Bev O’Cain, <strong>Health</strong>link South<br />
Brian Walden, Good <strong>Health</strong> Wanganui<br />
Helen Watson, HFA<br />
Marjet Pot, Auckland <strong>Health</strong>care<br />
Waiting Times Project<br />
Brett Solvander, HFA<br />
Erin Flood, HFA<br />
Gary Knighton, HFA<br />
Helen Williams, HFA<br />
Janice Kemp, HFA<br />
Marilyn Johnson, HFA<br />
Mark Batt, HFA<br />
Nigel Rickerby, HFA<br />
Philip Gander, HFA<br />
Ray Naden, HFA<br />
Valerie Meyer, HFA<br />
Vivienne Ong, HFA<br />
Nursing task<strong>for</strong>ce<br />
The HFA is trying to make policy changes to allow<br />
nurses to order lab and diagnostic tests and<br />
specialist referral rights and to allow nurses to<br />
purchase directly. Reprioritise <strong>for</strong> more Nurse-led<br />
services. Encourage better use <strong>of</strong> Practice Nurses<br />
within PCOs. Reprioritise to provide training <strong>for</strong><br />
nurses in management and leadership. Also the<br />
HFA is trying to have more nursing advice into<br />
decision-making.<br />
Laura Lambie, HFA<br />
Marama Parore Katene, HFA<br />
Other work involves: repriortising <strong>for</strong> more nurseled<br />
services; encourage better use <strong>of</strong> practise nurses<br />
within primary care organisations; provide training<br />
<strong>for</strong> nurses in management and leadership; have<br />
more nursing advice into decision-making.<br />
HFA Improving Our <strong>Health</strong> 55
<strong>Health</strong> — What’s Driving the Future<br />
The past decade has seen new health providers,<br />
particularly Maori, Pacific Islands communitybased<br />
and independent health providers become<br />
involved in servicing the health needs <strong>of</strong> our<br />
population.<br />
The healthcare provider market has changed<br />
markedly from what it was 10 years ago, primarily<br />
due to the introduction <strong>of</strong> the purchaser-provider<br />
split, and the opportunities this presented <strong>for</strong> new,<br />
diverse providers to enter the healthcare market.<br />
This change had the benefit <strong>of</strong> increasing the<br />
choices and methods <strong>of</strong> service delivery <strong>for</strong><br />
patients, but also led to greater fragmentation.<br />
More recently there has been a leaning more<br />
towards management <strong>of</strong> providers by the HFA and<br />
the Personal <strong>Health</strong> group with the aim <strong>of</strong><br />
improving integration and collaboration among the<br />
health providers at local level, in order that patients<br />
might benefit.<br />
The benefits can now been seen in the mix and<br />
choice <strong>of</strong> health providers the public and patients<br />
have access to. This situation is very different from<br />
what existed be<strong>for</strong>e.<br />
There are now more community and locallymanaged<br />
provider organisations, more Maori and<br />
Pacific Islands provider organisations which<br />
previously did not exist, and more multidisciplinary<br />
approaches to care. Care is less medically-centred,<br />
more holistic and focused on patient selfmanagement<br />
and in<strong>for</strong>med choice, through health<br />
education and prevention strategies.<br />
Managing groups <strong>of</strong> providers requires increased<br />
organisation <strong>of</strong> care <strong>for</strong> consumers. Organisations<br />
delivering healthcare seek opportunities <strong>for</strong> greater<br />
efficiency. The HFA seeks greater value <strong>for</strong> money<br />
and accountability <strong>for</strong> the public spend on behalf<br />
<strong>of</strong> the Government, while ensuring quality and<br />
equity standards are consistent and maintained.<br />
At the same time, the sector and public <strong>of</strong><br />
New Zealand, who are becoming better in<strong>for</strong>med<br />
year by year, are pressuring the sector to provide<br />
more evidence around their care decisions, and<br />
more certainty about what they can expect from<br />
the public health system.<br />
The trends in the health work<strong>for</strong>ce are also<br />
changing. For example, the makeup <strong>of</strong> the GP<br />
work<strong>for</strong>ce is changing with the age structure<br />
decreasing. Figures show that the numbers <strong>of</strong> GPs<br />
under 45 years <strong>of</strong> age increased from 35.6 percent<br />
in 1980 to 61.7 percent in 1995. 1 There are higher<br />
numbers <strong>of</strong> female practitioners in part time<br />
practice, and there is a growing number <strong>of</strong> Maori<br />
practitioners – estimated to be around 200 in 1998 2 .<br />
The nursing work<strong>for</strong>ce is changing. An increasing<br />
number <strong>of</strong> nurses are working part-time, and<br />
working <strong>for</strong> different types <strong>of</strong> providers rather than<br />
the historical pattern <strong>of</strong> working <strong>for</strong> hospitals or<br />
GP-based practices. Some are <strong>for</strong>ming independent<br />
nursing organisations to provide care in the home<br />
and community, while others are being attracted<br />
to Maori and Pacific Islands health providers.<br />
Population and Demographic Trends<br />
The Personal <strong>Health</strong> group believes that<br />
demographic and related social trends will drive<br />
future change in the provision <strong>of</strong> health care,<br />
including:<br />
• Increasing total population: a projected increase<br />
from 3,714,000 in 1996 to 4,232,000 in 2021,<br />
mainly due to immigration and mostly in the<br />
North Island.<br />
• Increasing urbanisation, which has implications<br />
<strong>for</strong> the viability <strong>of</strong> rural healthcare and pressures<br />
urban services<br />
• Increasing ageing population, with numbers <strong>of</strong><br />
elderly people projected to outnumber children<br />
by 2031<br />
• Declining birth rate, with the proportion <strong>of</strong><br />
children in the population expected to decline<br />
from 23 percent in 1994 to 18 percent by 2031<br />
• Steady growth in the Maori population from<br />
434,000 in 1991 to 546,000 in 2016. At least<br />
84 percent <strong>of</strong> this growth will be in the North<br />
Island. Though improving, Maori are likely to<br />
continue to have lower socio-economic status<br />
and higher morbidity rates than experienced by<br />
the rest <strong>of</strong> the population. Maori population<br />
currently accounts <strong>for</strong> 15 percent <strong>of</strong> the NZ<br />
population.<br />
56
• Steady growth in the Pacific Islands population<br />
from 4 percent <strong>of</strong> the population in 1991 to 7<br />
percent in 2031<br />
(Source: Statistics New Zealand Demographic<br />
Trends 1998)<br />
These demographic trends will likely lead to a<br />
growth in the need <strong>for</strong> primary and secondary care,<br />
especially among the elderly and those with low<br />
incomes.<br />
As Maori and Pacific Islands populations grow, so<br />
will the need <strong>for</strong> enhanced services which more<br />
appropriately meet their needs. This will include<br />
a need <strong>for</strong> more healthcare services delivered and<br />
managed by Maori and Pacific Islands providers,<br />
including strategic and policy development around<br />
those services.<br />
The growing pressure from these communities to<br />
participate in the decision-making and delivery<br />
process has implications <strong>for</strong> the public sector<br />
infrastructure, and is a trend that the Personal<br />
<strong>Health</strong> group has been actively attempting to<br />
cater to.<br />
<strong>Health</strong> Status and Service Use<br />
New patterns <strong>of</strong> disease and changing patterns <strong>of</strong><br />
existing diseases will continue to drive the<br />
healthcare sector. Particularly important is the<br />
increasing incidence <strong>of</strong> some infectious diseases as<br />
a result <strong>of</strong> antibiotic resistance and low socioeconomic<br />
status (e.g. living conditions, income<br />
levels) as well as age-related illness, chronic diseases<br />
and mental illness.<br />
The key determinants <strong>of</strong> health status are ageing,<br />
changing ethnicity, lifestyle choices, income and<br />
education, and the state <strong>of</strong> the environment.<br />
1 Clinical Training Agency 1995<br />
2 Personal communication, Te Ohu Rata o Aotearoa (Maori<br />
Medical Association)<br />
For more in<strong>for</strong>mation you can contact the HFA’s in<strong>for</strong>mation freephone on:<br />
0800 ENQUIRE (0800 367 8473).<br />
Alternatively, you may wish to visit our website at:<br />
http://www.hfa.govt.nz<br />
The HFA also runs a freephone number <strong>for</strong> in<strong>for</strong>mation about Maternity Services:<br />
0800 MUM 2 BE (0800 686 223).